Downloaded 129 times

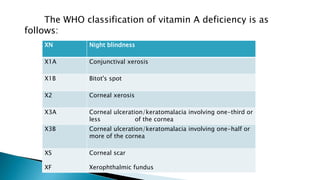

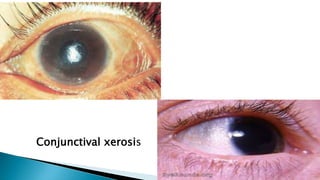

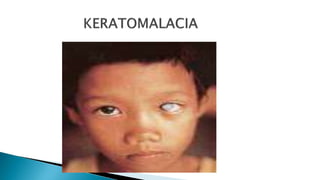
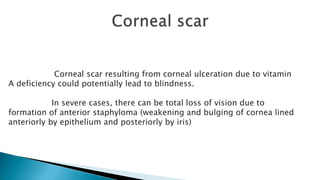



Vitamin A deficiency can cause various ocular manifestations known as xerophthalmia, ranging from mild conjunctival dryness to the severe complication of keratomalacia, which can lead to blindness. Early signs include night blindness and Bitot's spots on the conjunctiva. Prolonged deficiency can cause keratomalacia, in which the cornea develops ulcers and thinning. Treatment involves high-dose oral or injected vitamin A supplementation.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












