Downloaded 781 times


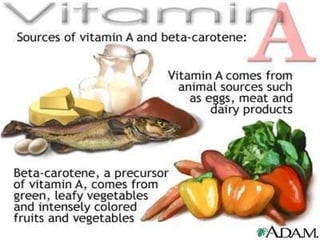
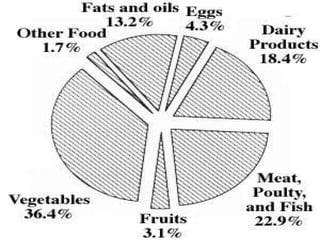


Vitamin A is essential for normal body functions like vision, cellular integrity, immune function and growth. It is found naturally in animal foods like liver, egg yolks, and dairy products as well as plant foods like spinach, carrots and mangoes. Vitamin A deficiency can cause night blindness and dryness of the eyes and later corneal ulceration and blindness if left untreated. Early signs are diagnosed through eye examinations and blood tests while more advanced cases show skin and respiratory issues. Deficiency is treated with high oral or injectable vitamin A supplements depending on severity. Prevention involves breastfeeding, vitamin A supplements with vaccines and adequate nutrition.