Download to read offline

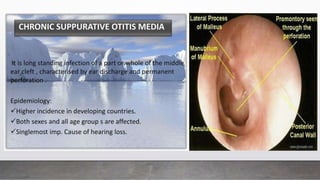
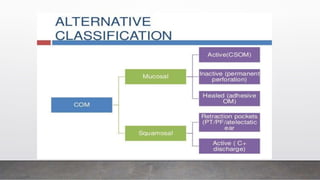
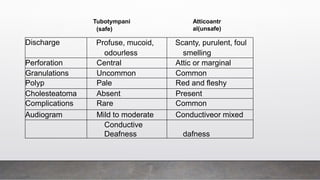
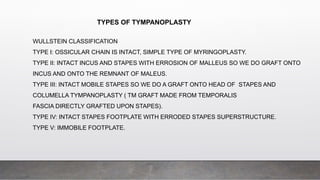
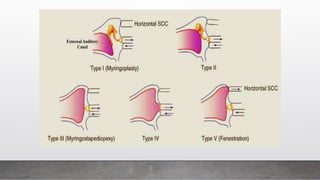
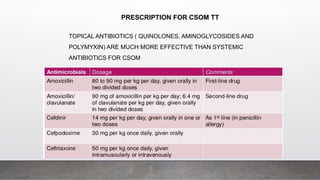
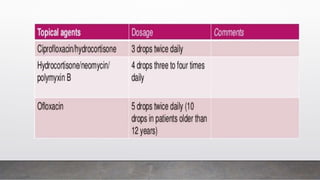


Chronic Suppurative Otitis Media (CSOM) is classified into two types: tubotympanic (safe) and atticoantral (unsafe), with the latter having a higher risk of complications. The document outlines the etiology, pathology, clinical features, and management plan for CSOM, emphasizing the importance of controlling infection and addressing hearing loss. It also describes the types of tympanoplasty and provides guidance on clinical investigation and treatment strategies.

















































![Down syndrome (2)[1].pptx pediatric lecture](https://cdn.slidesharecdn.com/ss_thumbnails/downsyndrome21-240709094926-fcdd02d9-thumbnail.jpg?width=640&height=640&fit=bounds)










![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)


























