Downloaded 668 times
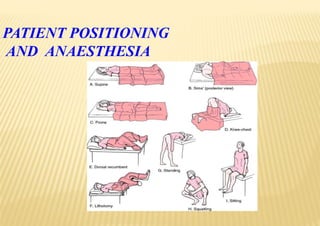
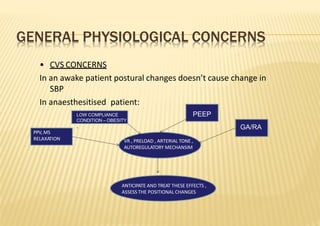
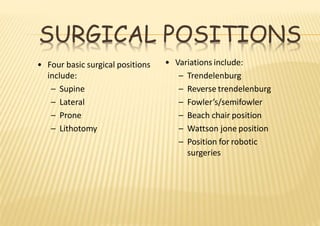


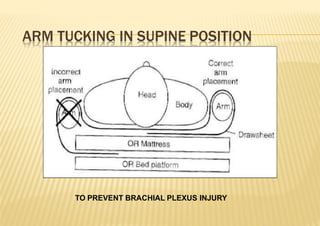
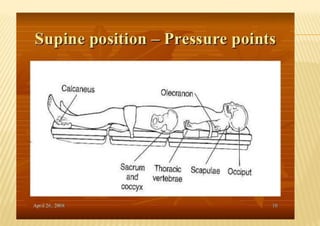

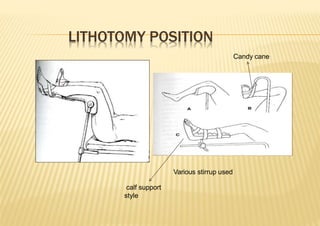
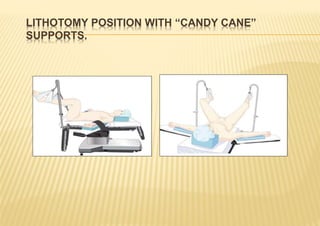
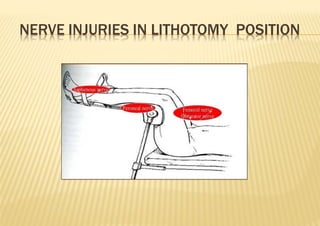

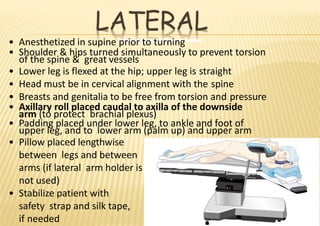
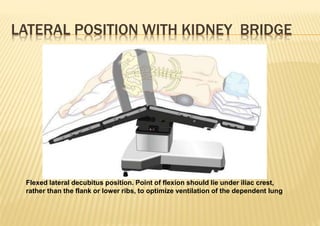
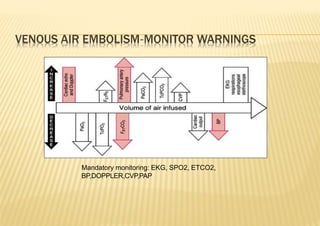
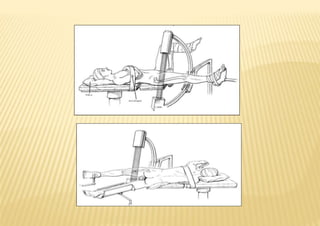
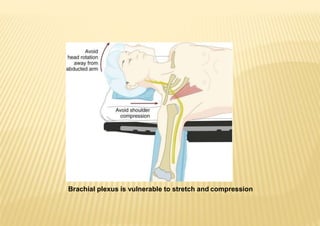
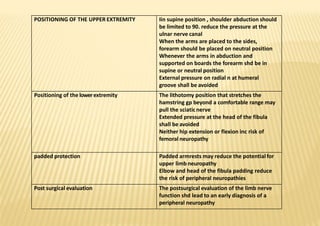

The document discusses patient positioning considerations for anesthesia. It notes that positioning is a joint responsibility of the surgeon and anesthesiologist to balance surgical needs with risks to the patient. Key positions discussed include supine, lateral, prone, lithotomy, and variations like Trendelenburg. Physiological concerns for each position are outlined such as effects on circulation, pulmonary function, and nerve injuries. Proper padding and stabilization are emphasized to prevent pressure injuries.



































































