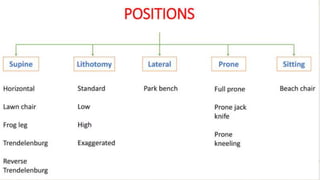
The document provides a comprehensive overview of patient positioning during surgical procedures, emphasizing the responsibility of the medical team to ensure optimal positioning that balances surgical needs and patient safety. It details various positioning strategies, associated physiological changes, potential complications, and best practices to prevent adverse outcomes such as nerve injuries and pressure sores. Key positions discussed include supine, lithotomy, lateral, prone, and sitting, along with considerations for padding and support to maintain patient comfort and safety.