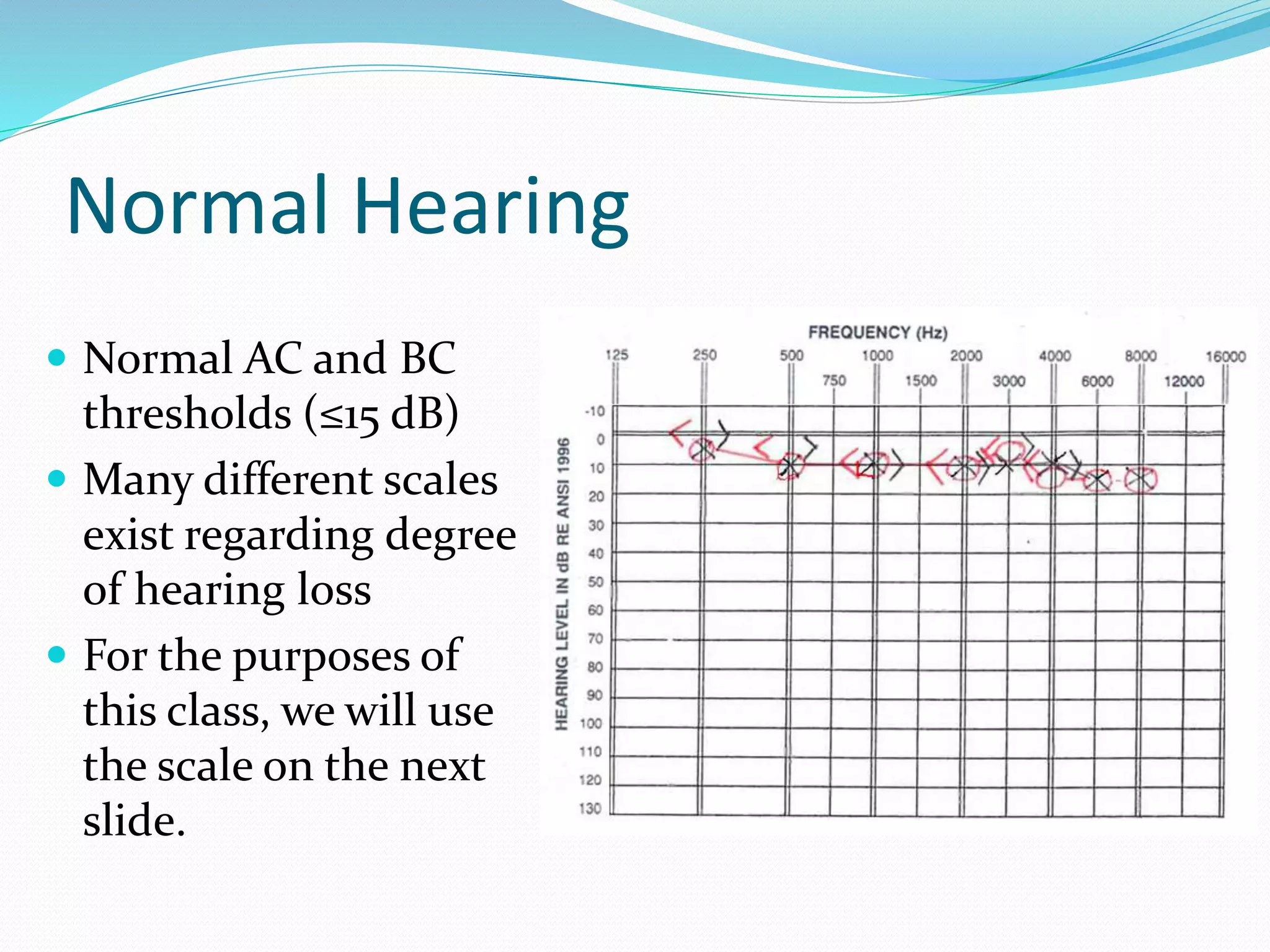
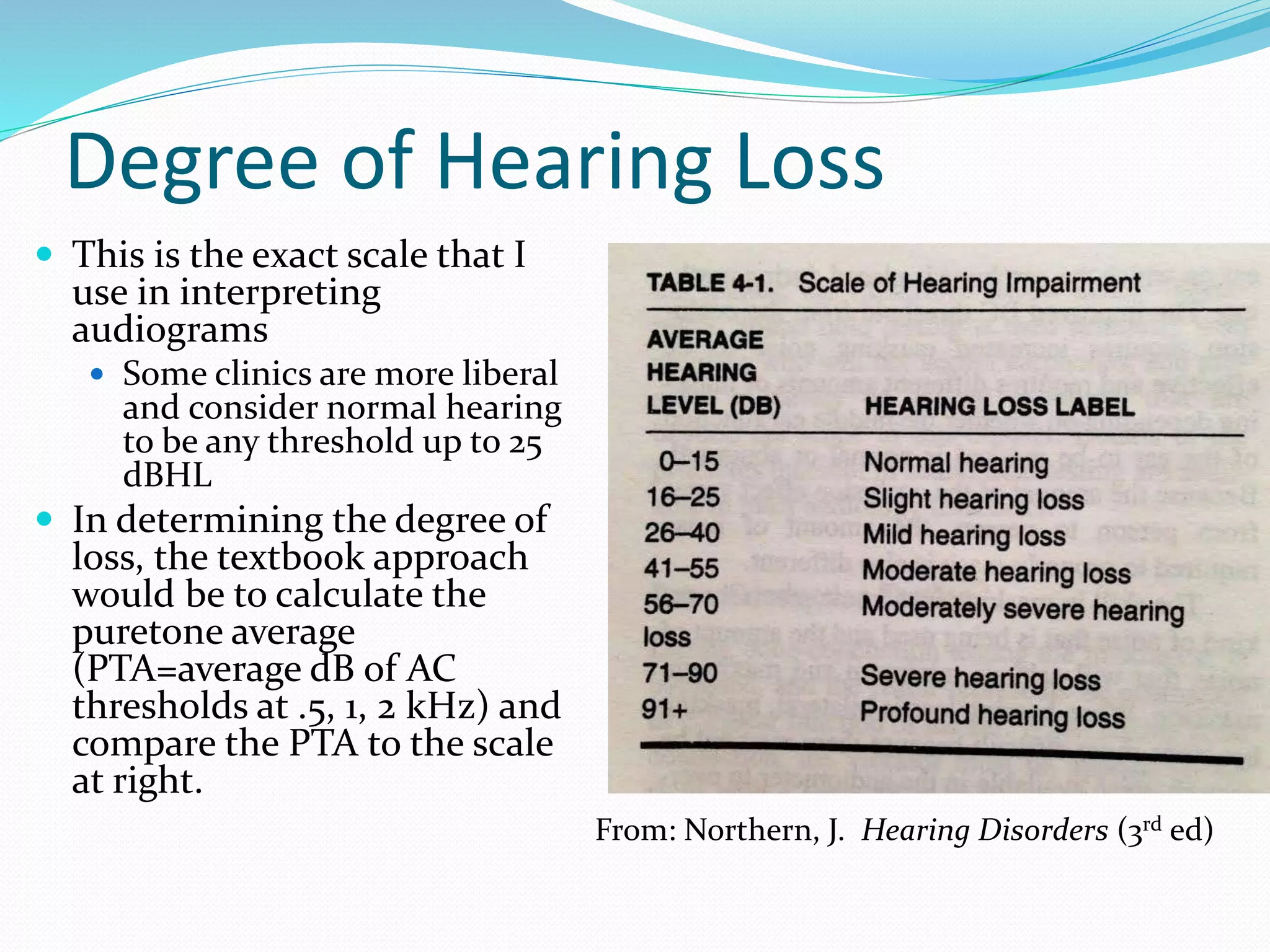
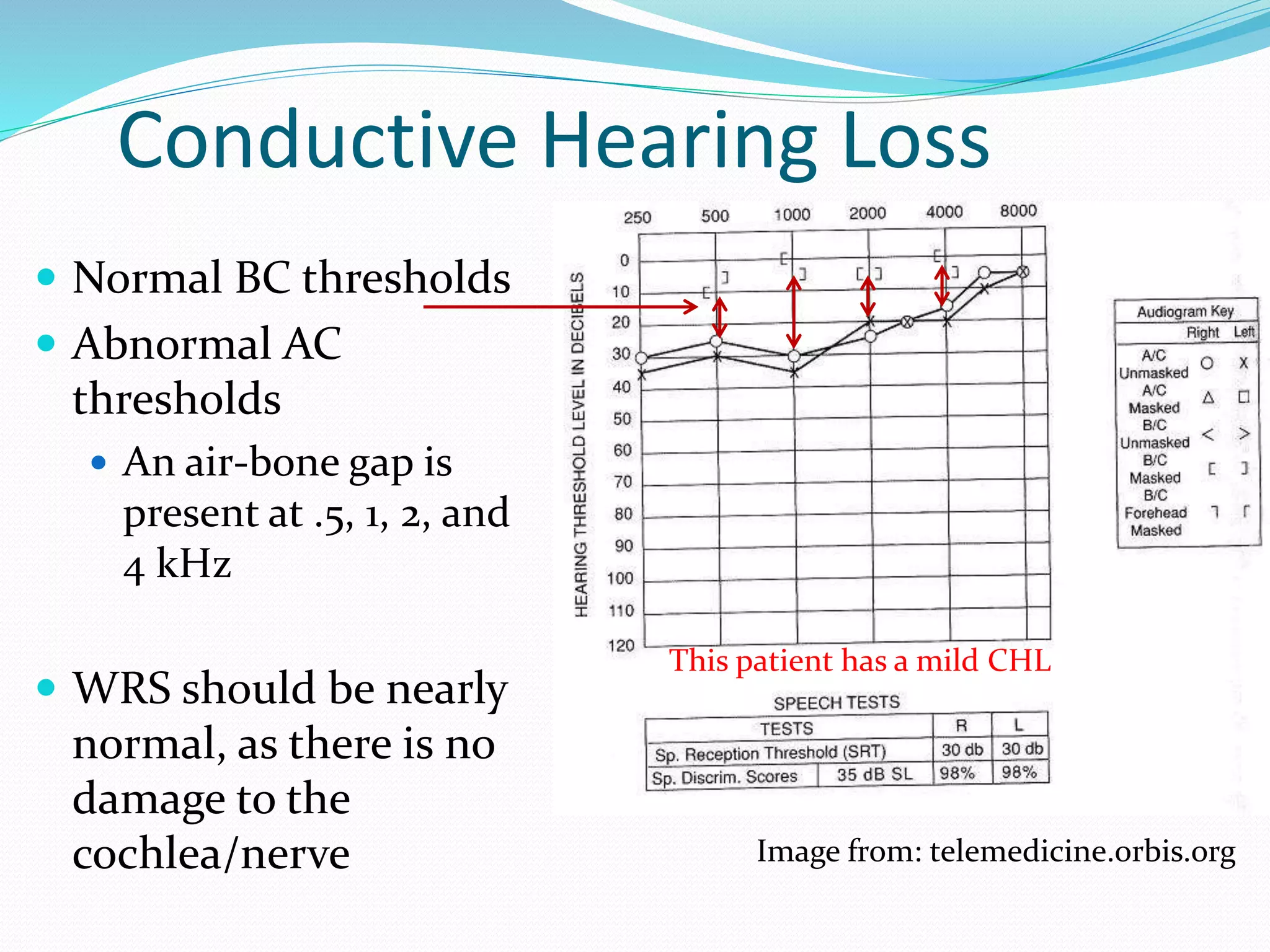
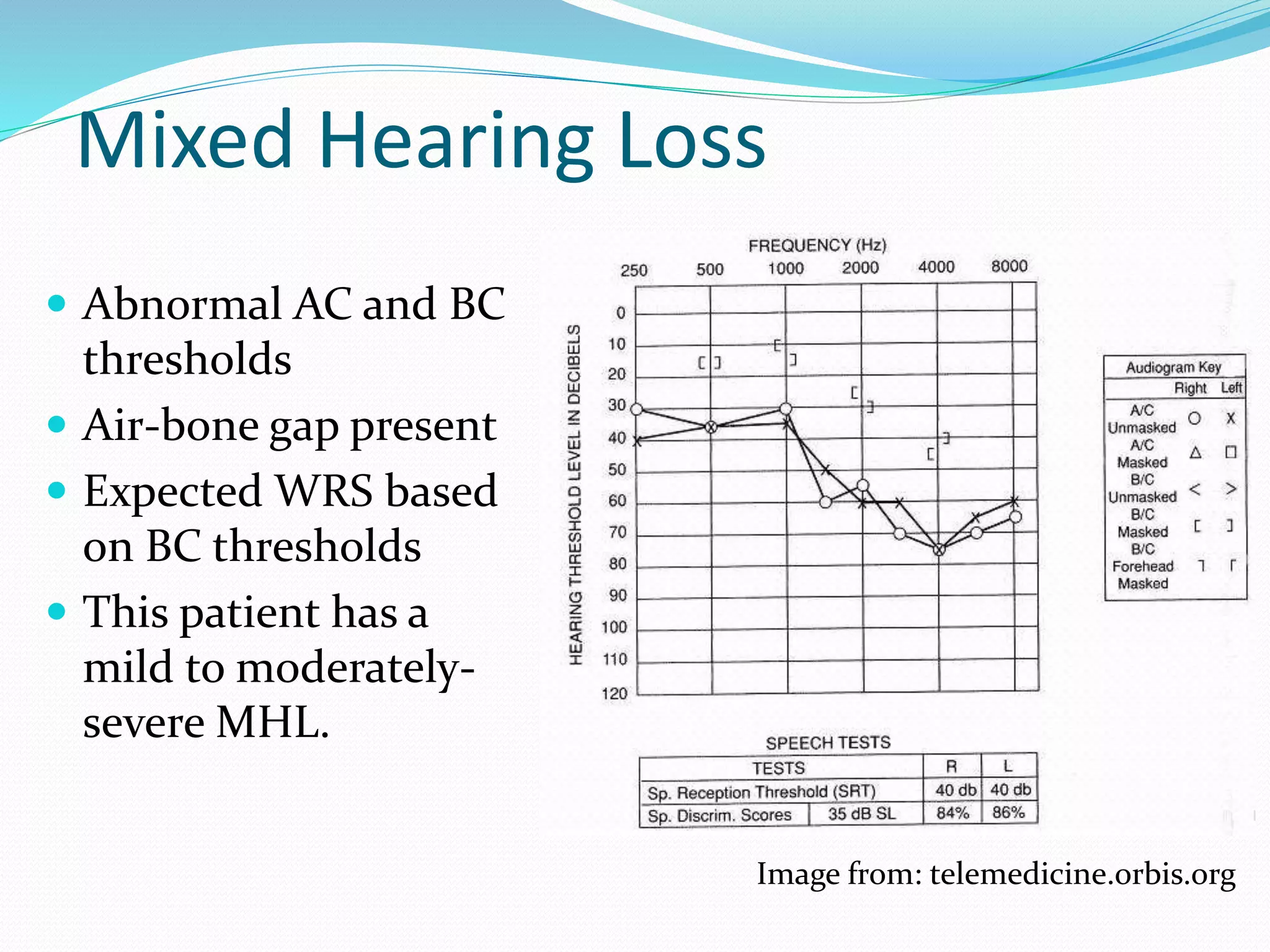
This document defines different types of hearing loss including conductive, sensorineural, and mixed. It describes the magnitude, type, and configuration of hearing loss. Normal hearing is defined as thresholds ≤15 dB. Degree of loss is categorized as slight, mild, moderate, etc. based on puretone average. Conductive loss shows normal bone conduction but abnormal air conduction with an air-bone gap. Sensorineural loss has equal abnormal air and bone conduction thresholds. Mixed loss has characteristics of both. Configuration can be flat, rising, sloping, or precipitous. Certain conditions require medical referral.