Download to read offline









![Pure-Tone Bone-Conduction Testing
Pure-tone bone-conduction
thresholds provide auditory
threshold information when the
cochlea is stimulated more or less
directly, with stimuli bypassing
external and middle ear structures.
Differences between thresholds
obtained through air and bone
conduction are used to determine
the type of hearing loss (normal
hearing versus conductive loss
versus sensorineural hearing loss
[SNHL]) and the magnitude of
conductive hearing loss if it exists.](https://image.slidesharecdn.com/diagnosticaudiologyaudiometrytympanometryandoae-240401035023-2f38d330/75/diagnostic-audiology-audiometry-tympanometry-and-OAE-pptx-23-2048.jpg)
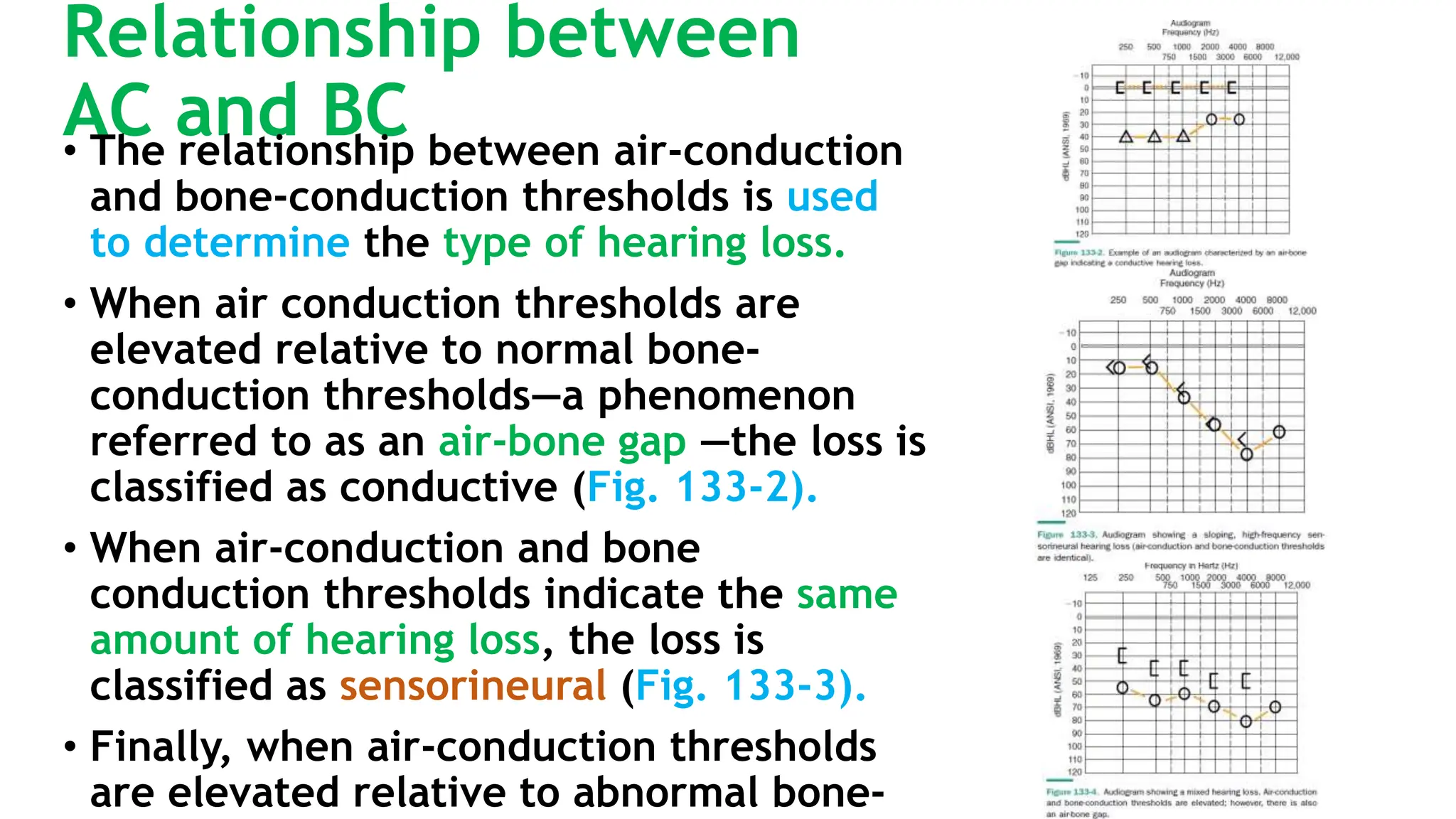

























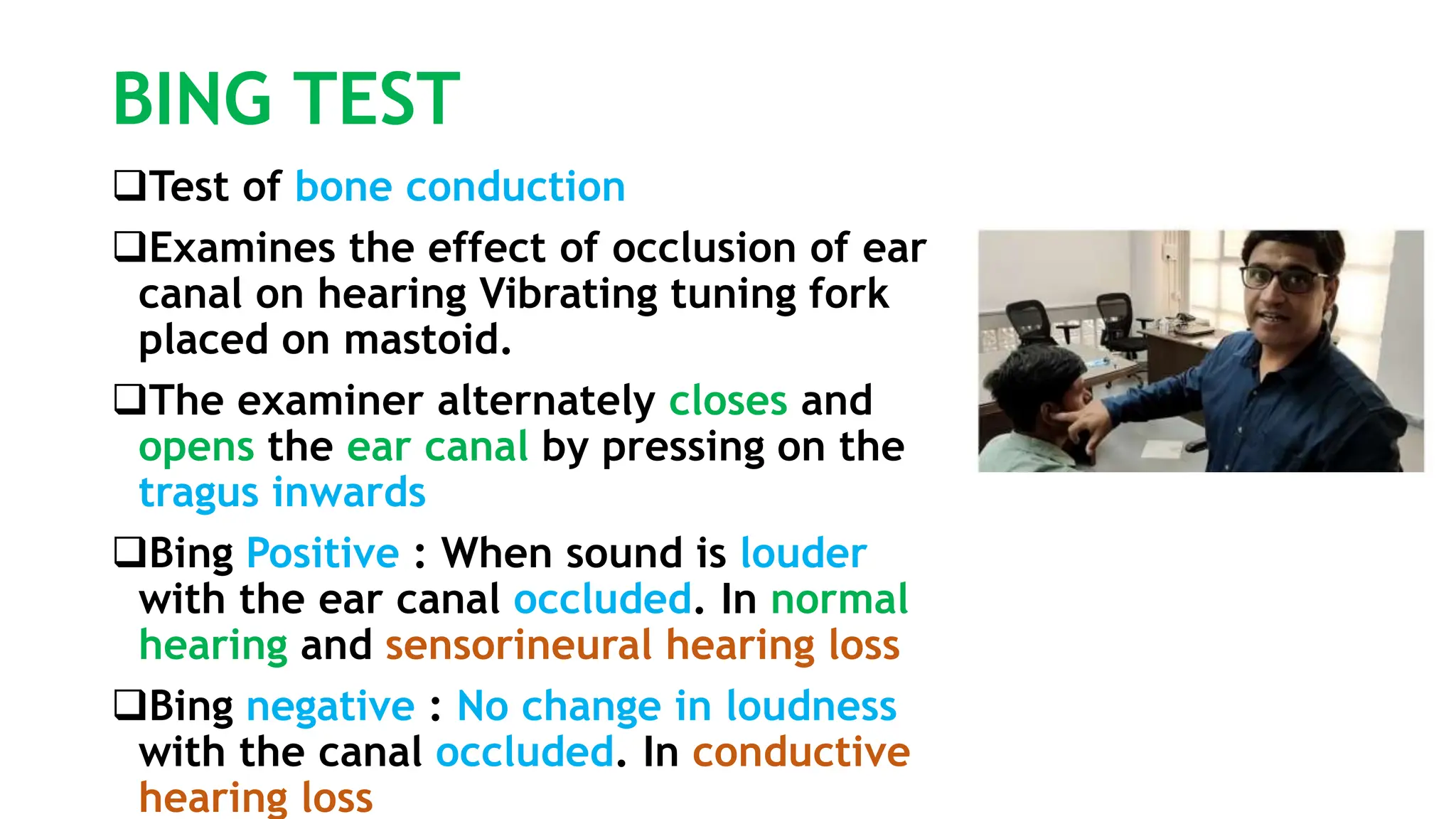
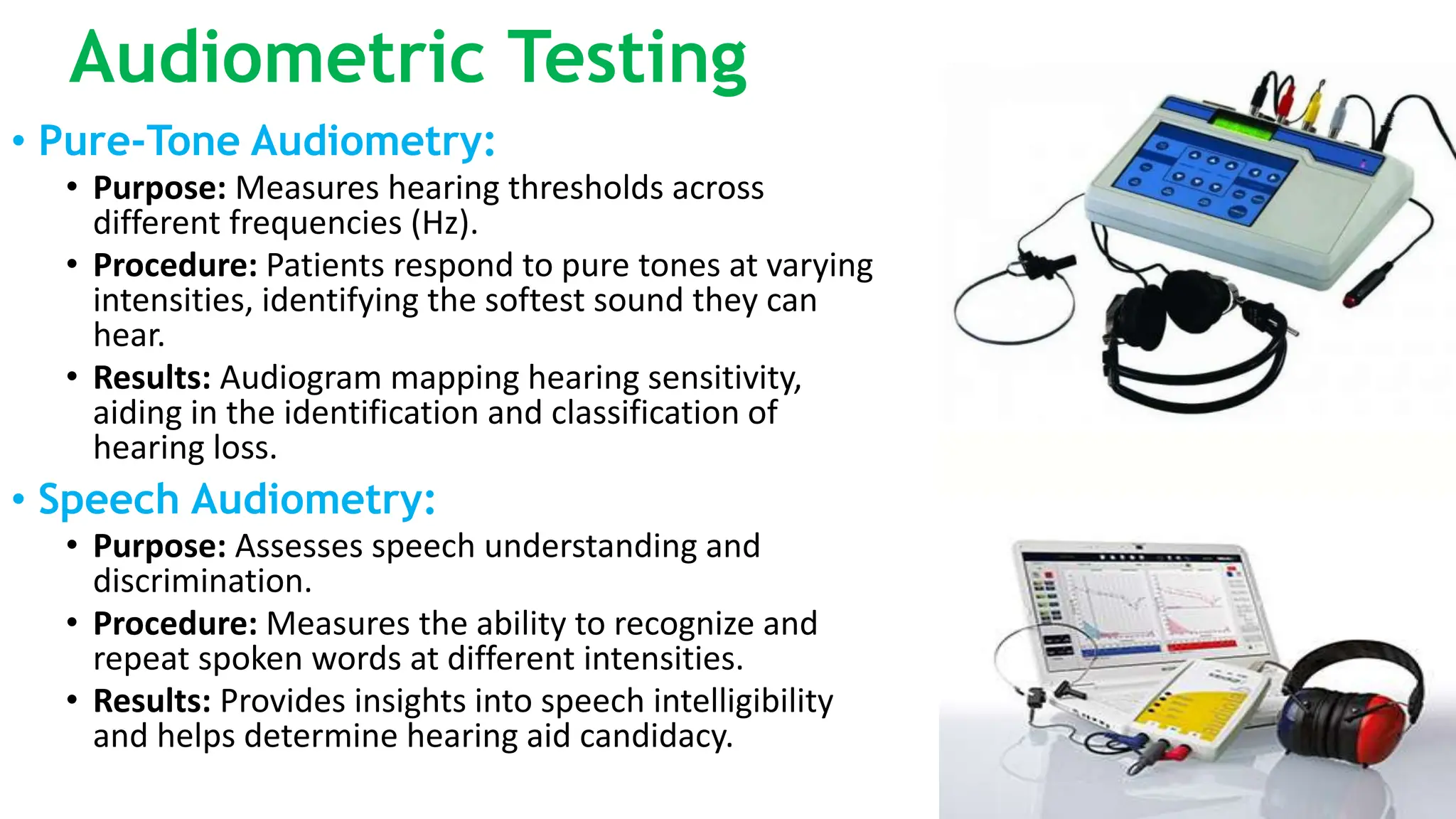
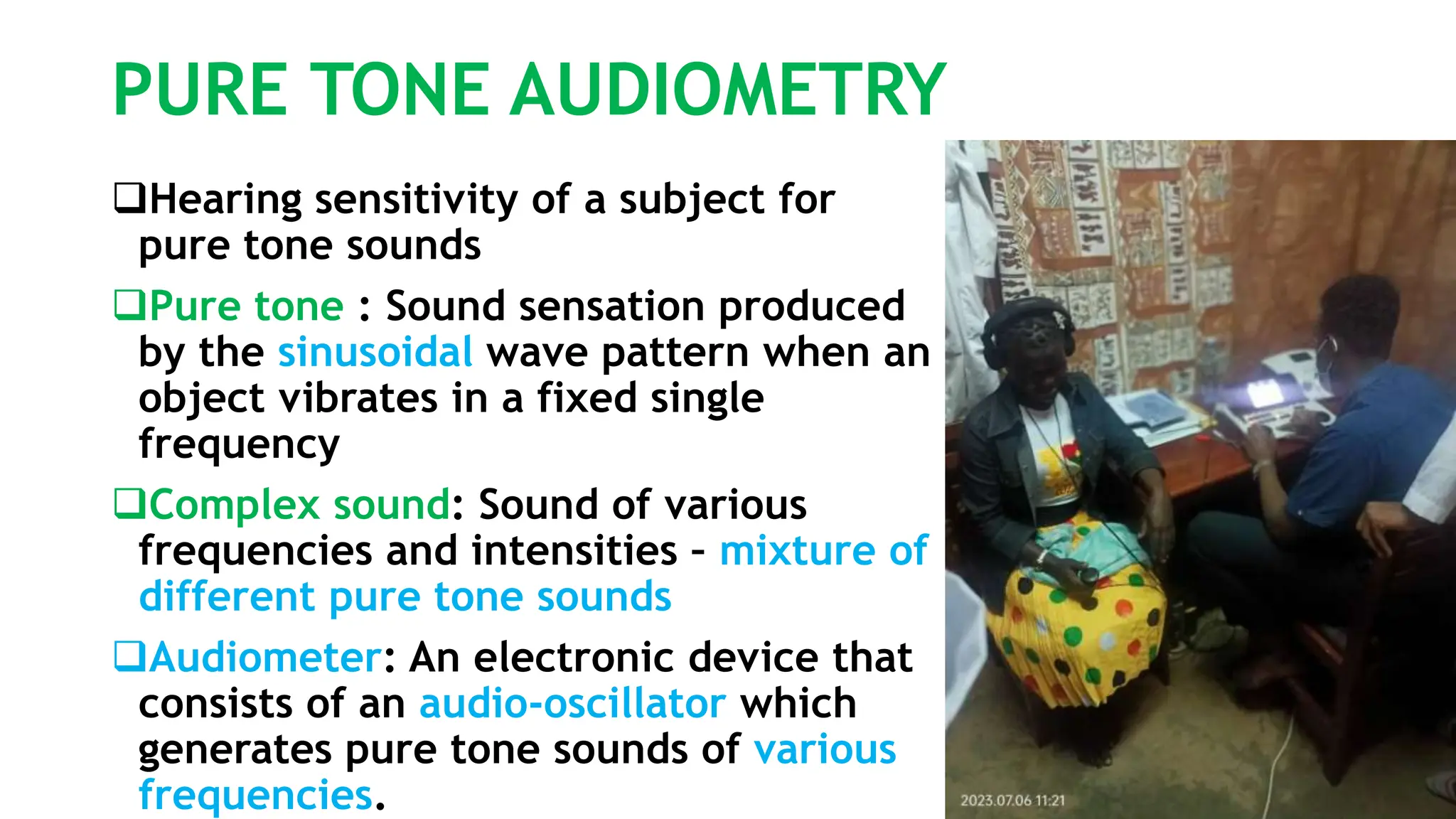
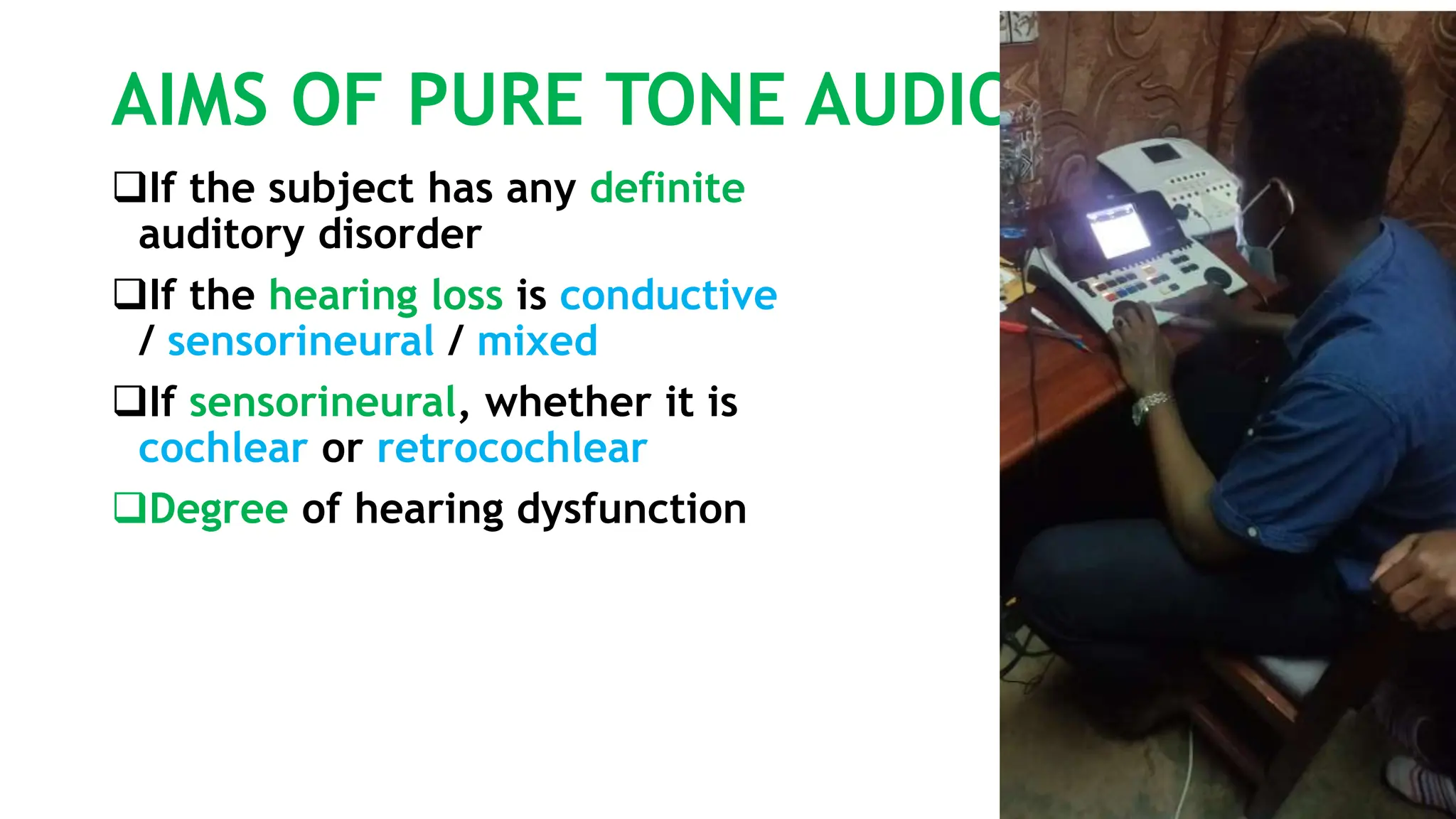
This document discusses diagnostic audiology techniques for assessing hearing and balance disorders. It describes both subjective tests like tuning fork tests and objective tests like pure tone audiometry. Tuning fork tests include Rinne's test, Weber's test, and others to qualitatively assess hearing loss type. Pure tone audiometry objectively measures hearing thresholds across frequencies to create an audiogram and diagnose hearing loss type and degree. Speech audiometry assesses speech understanding. Together these techniques provide diagnostic information about auditory function.







![Mai EchoG and OAEs ENT [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maiechogandoaesentrecovered-230503021828-debb4756-thumbnail.jpg?width=640&height=640&fit=bounds)



























































