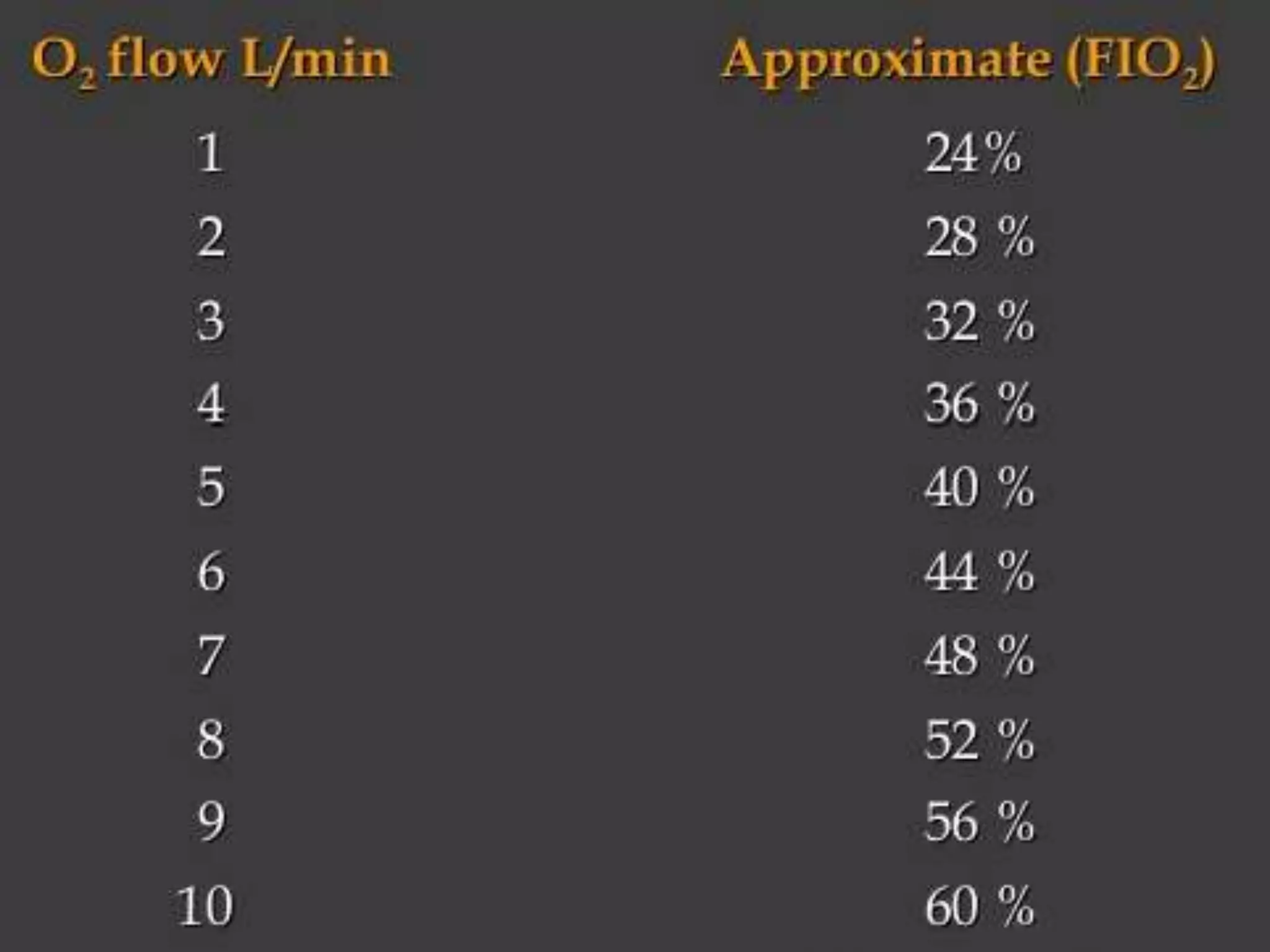
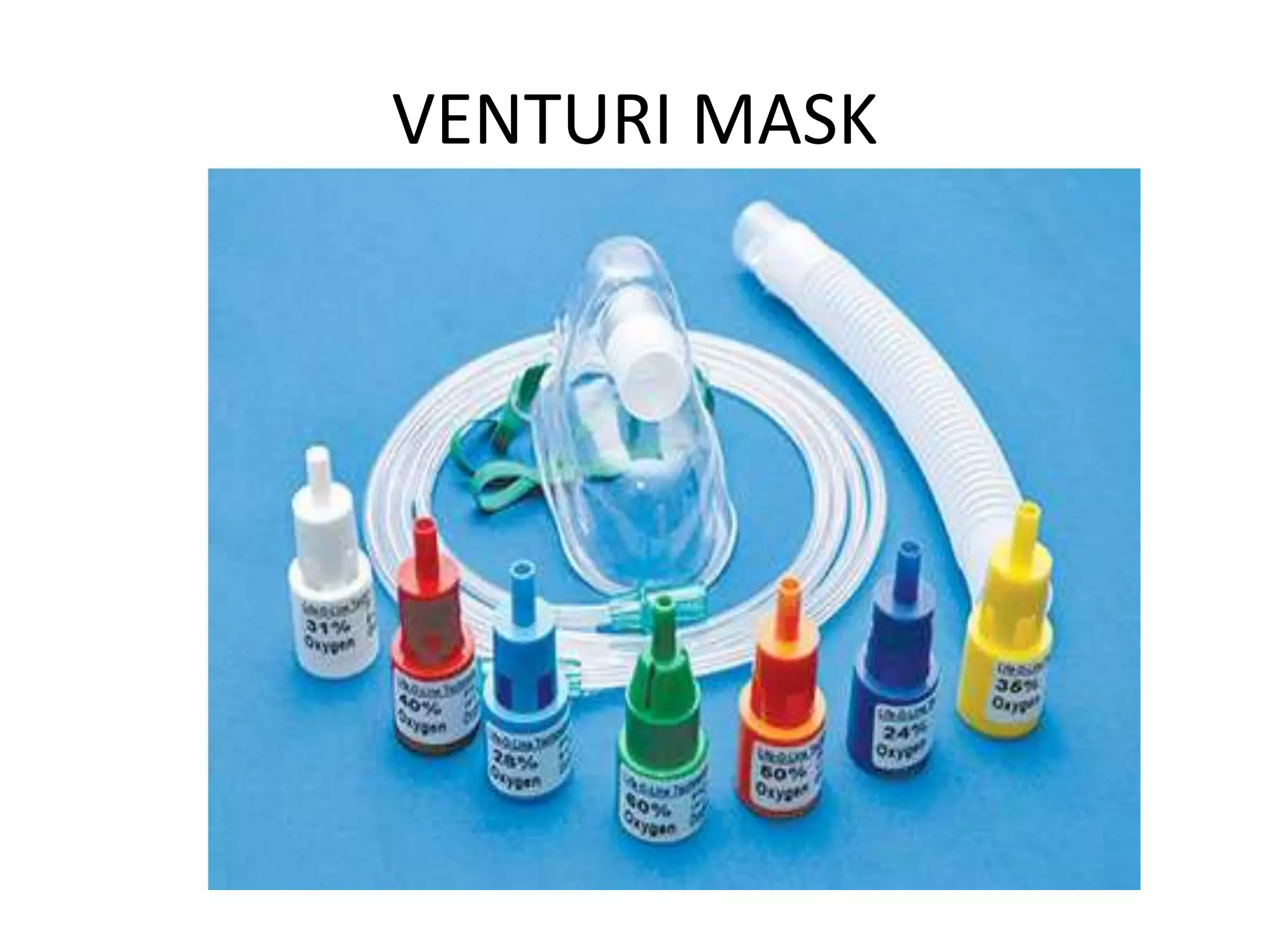
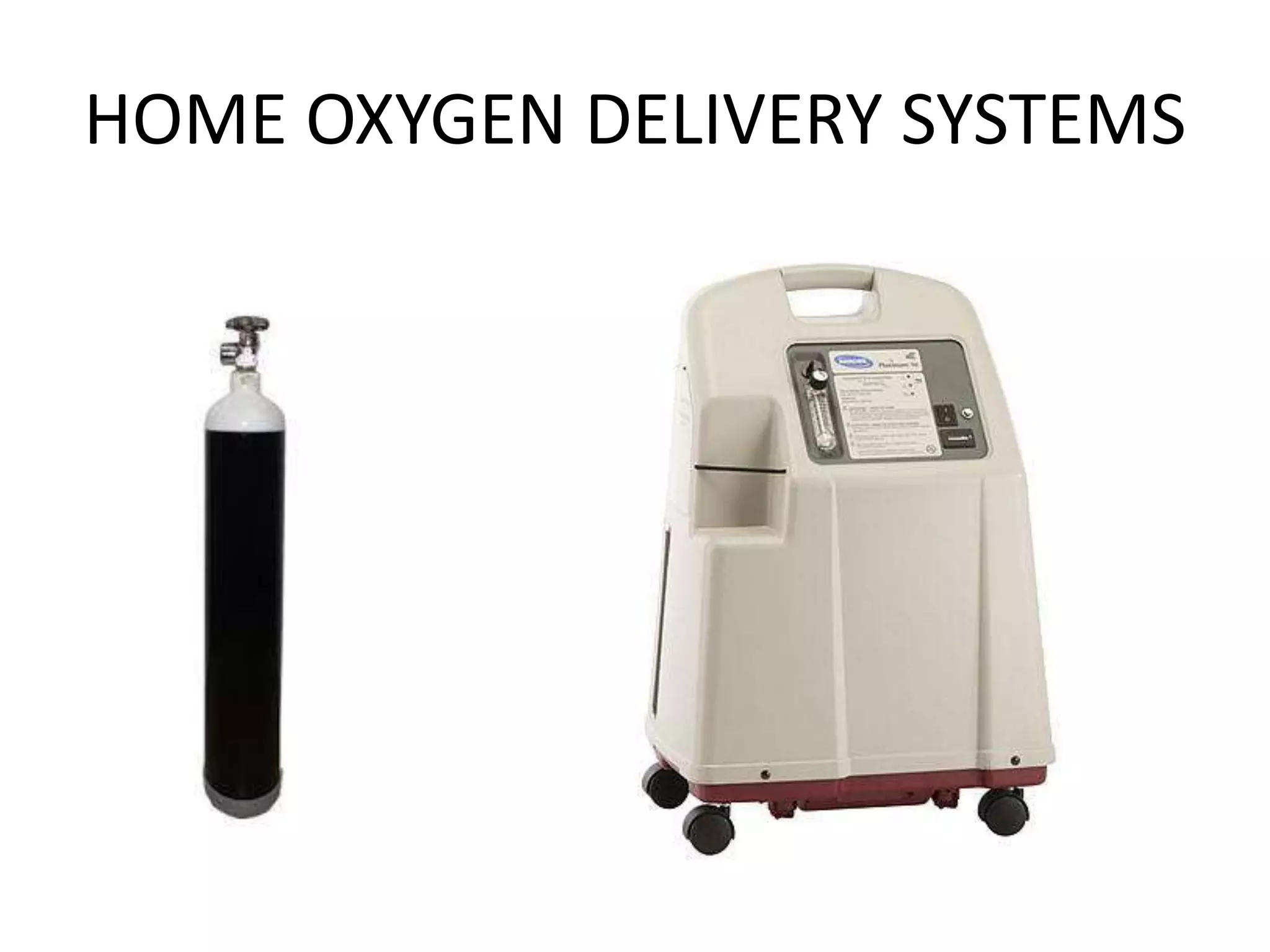
An oxygen delivery system administers oxygen to increase arterial oxygenation. Systems are classified as low-flow or variable-performance devices, and high-flow or fixed-performance devices. Low-flow devices include nasal cannulas and masks, which provide supplemental oxygen. High-flow devices like venturi masks, partial rebreather masks, and non-rebreather masks meet inspiratory demands and generate accurate oxygen concentrations. At home, oxygen is delivered via cylinders or concentrators, which remove nitrogen from room air to produce oxygen.