Downloaded 452 times
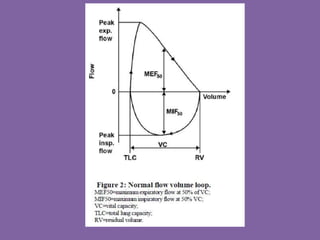
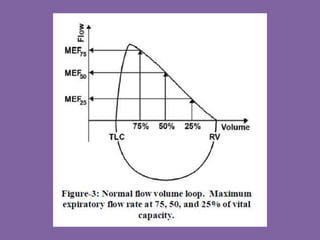

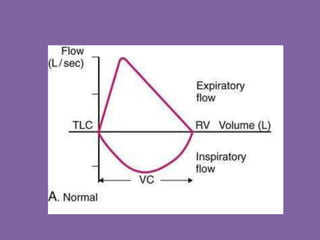
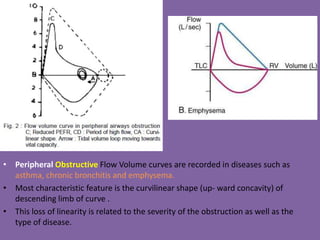
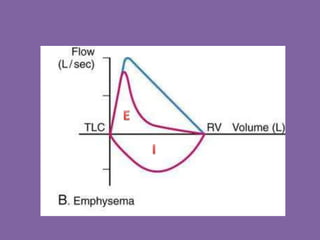

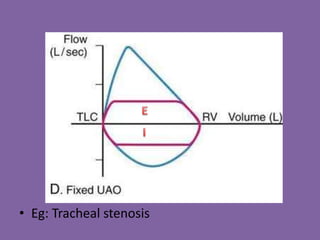
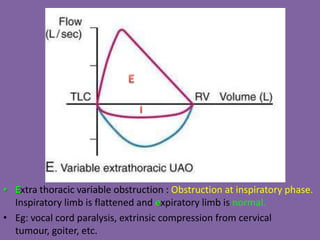
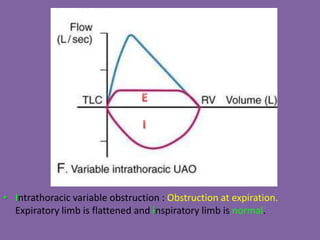
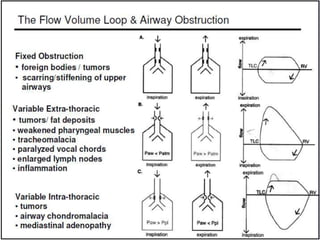
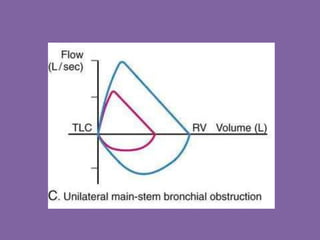
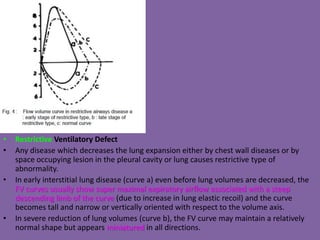
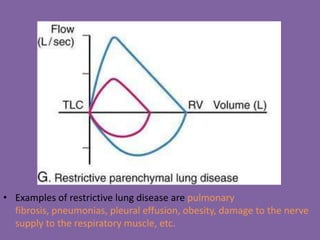
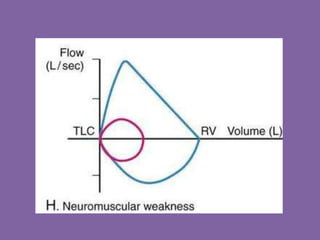
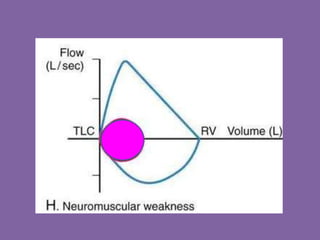
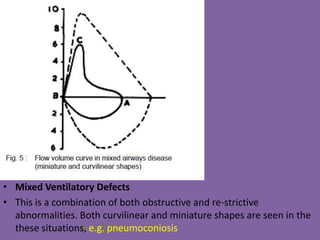
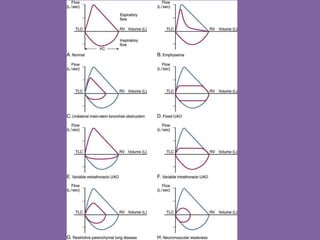
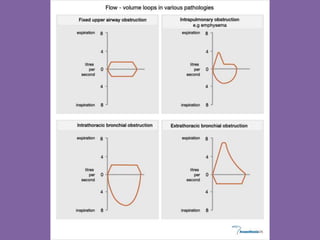
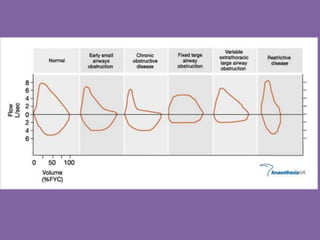
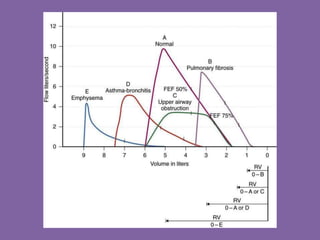


This document discusses pulmonary flow volume loops, which can identify obstructive or restrictive ventilatory defects. Obstructive defects cause the descending limb of the loop to have an upward concavity. Restrictive defects cause the loop to become tall and narrow or miniature in all directions. Specific loop patterns indicate fixed or variable upper airway obstruction, intrathoracic variable obstruction, or extrathoracic variable obstruction. Mixed defects show both curvilinear and miniature loop shapes. Examples of conditions that can cause these patterns are also provided.