Downloaded 202 times
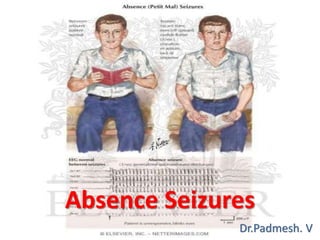
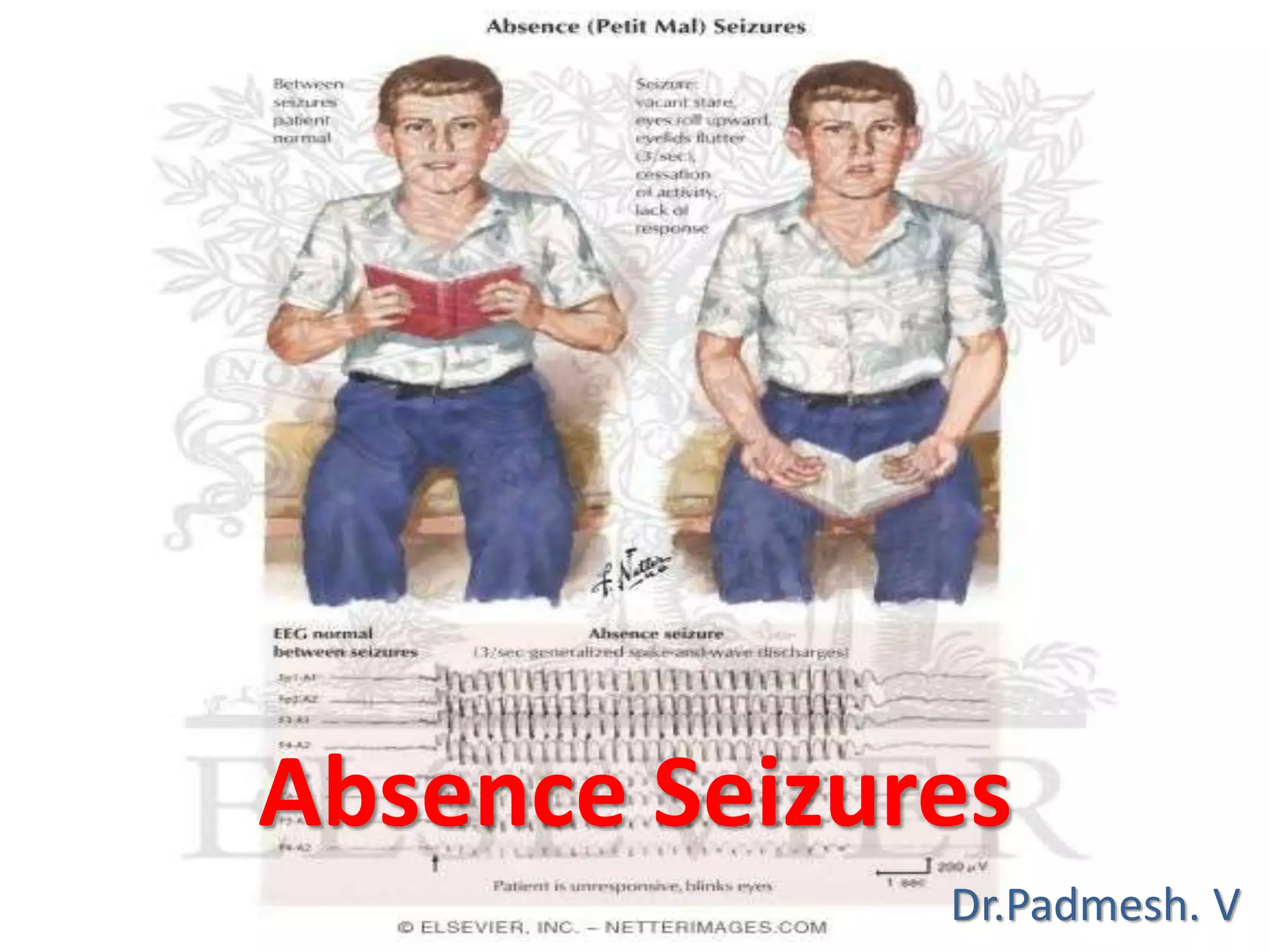
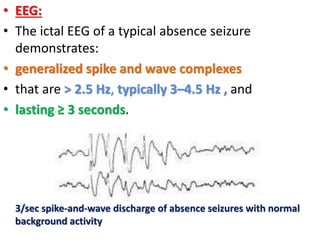


Absence seizures typically have two peaks in age of onset, between 5-8 years and near 12 years. Childhood absence epilepsy (CAE) accounts for 10-17% of childhood epilepsy cases and is characterized by brief seizures without aura or postictal period. Typical absence seizures involve eye blinking or movements lasting a few seconds accompanied by generalized spike-and-wave discharges on EEG. Treatment typically begins with ethosuximide, though valproate or lamotrigine may be used if generalized tonic-clonic seizures are also present. While often labeled benign, CAE has variable outcomes, with some studies finding generalized tonic-clonic seizures develop later in 40% of cases.



























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



