Downloaded 138 times







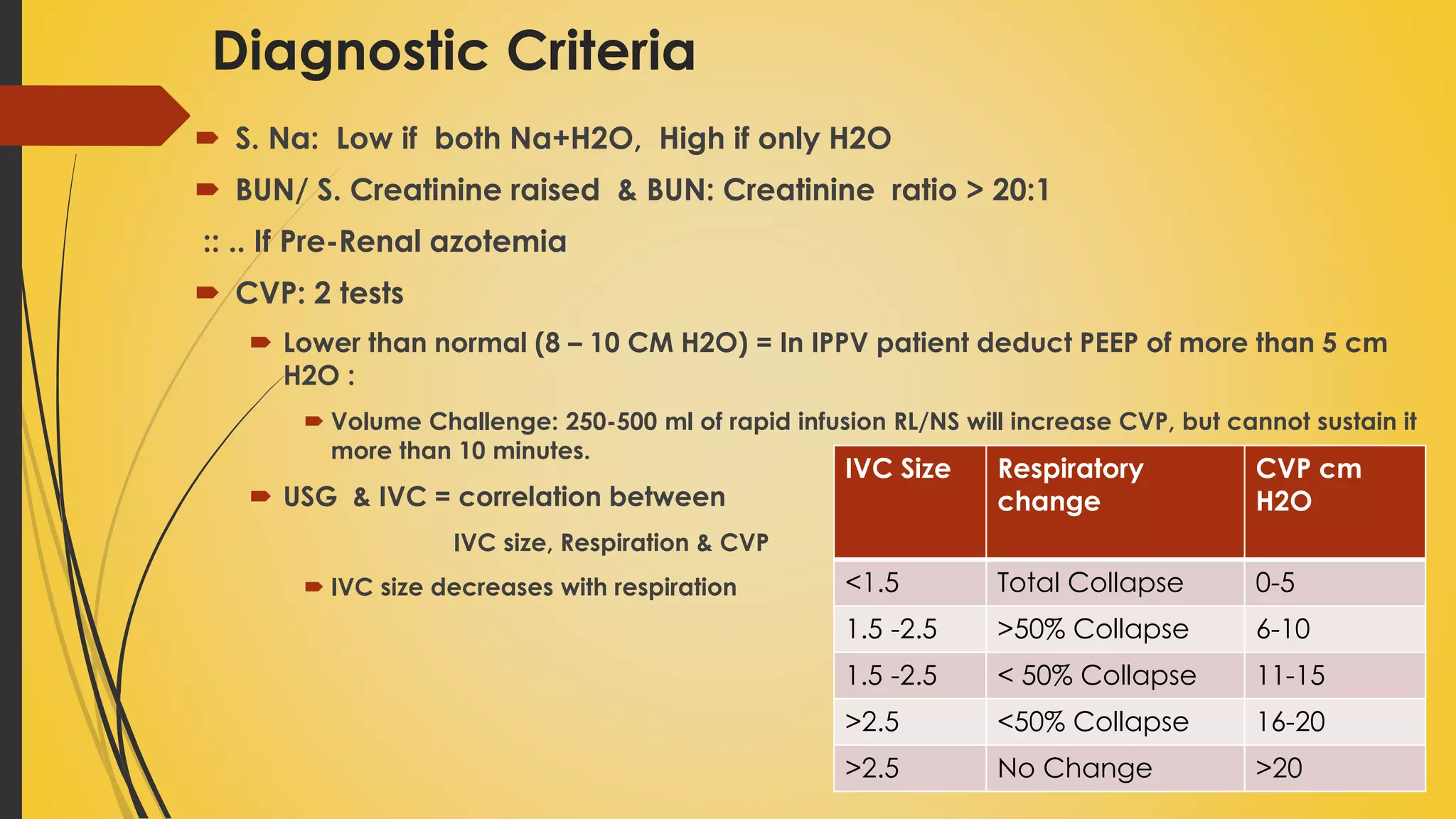







This document discusses fluid balance and fluid compartments in the human body. It defines key terms like total body water, extracellular fluid, intracellular fluid, osmolality, tonicity, electrolytes and explains the distribution and regulation of body water. It also describes hypovolemia, its causes, diagnostic criteria and management approaches for hemorrhagic and non-hemorrhagic hypovolemia. Common intravenous fluids are classified and their properties and uses are explained.
Highlights importance of water, defining it as vital for life and balancing pH and fluid levels.
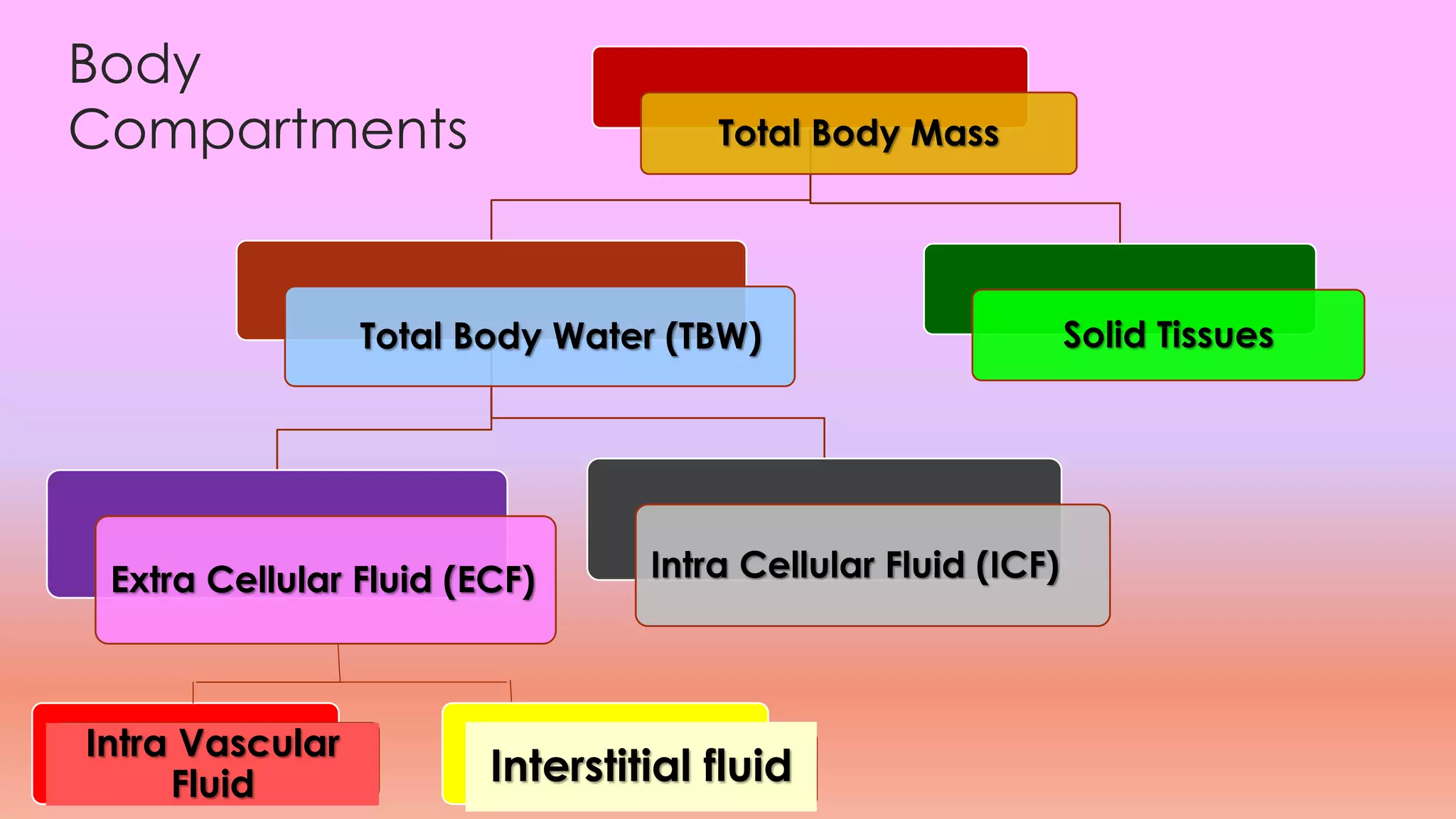
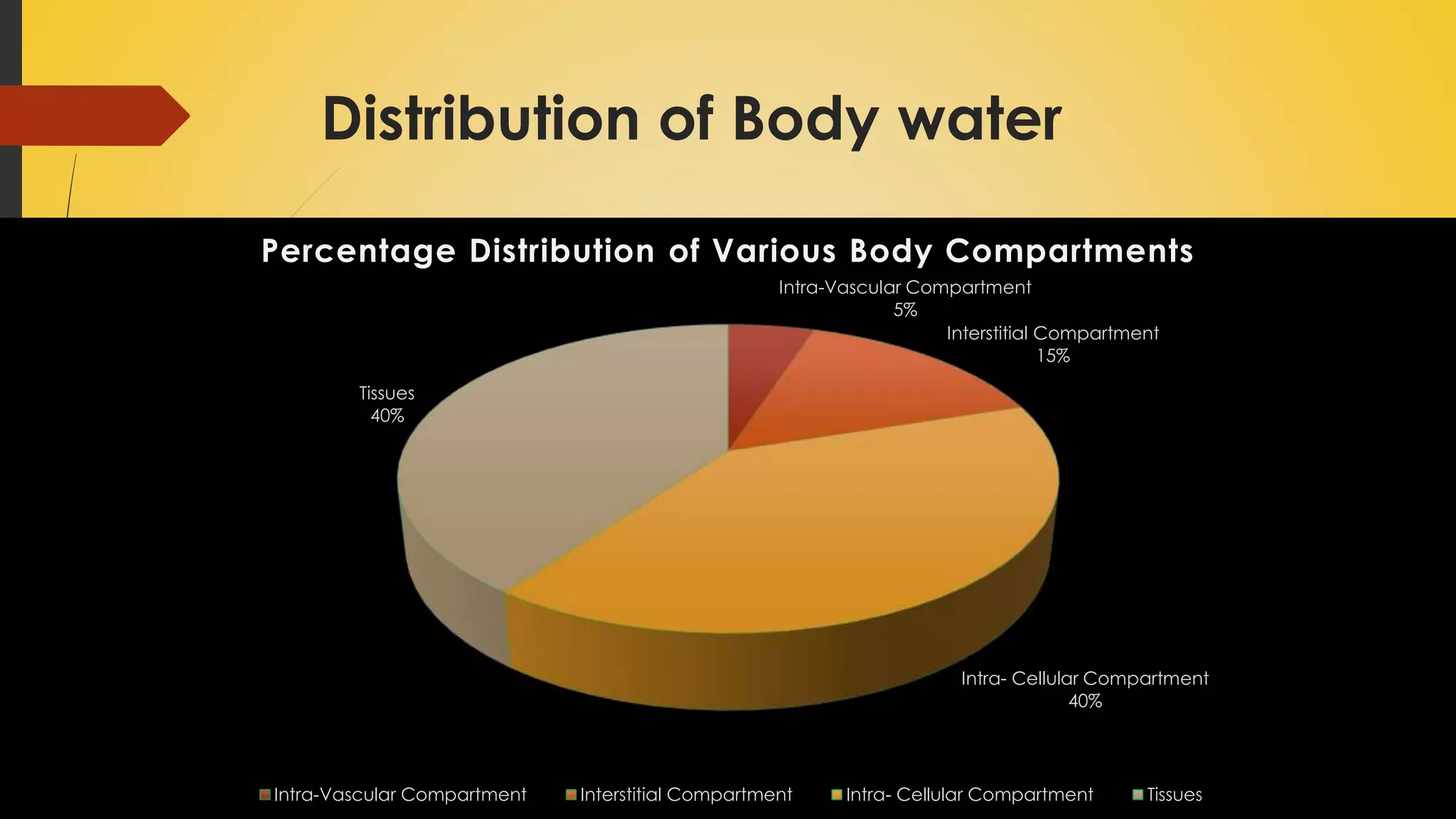
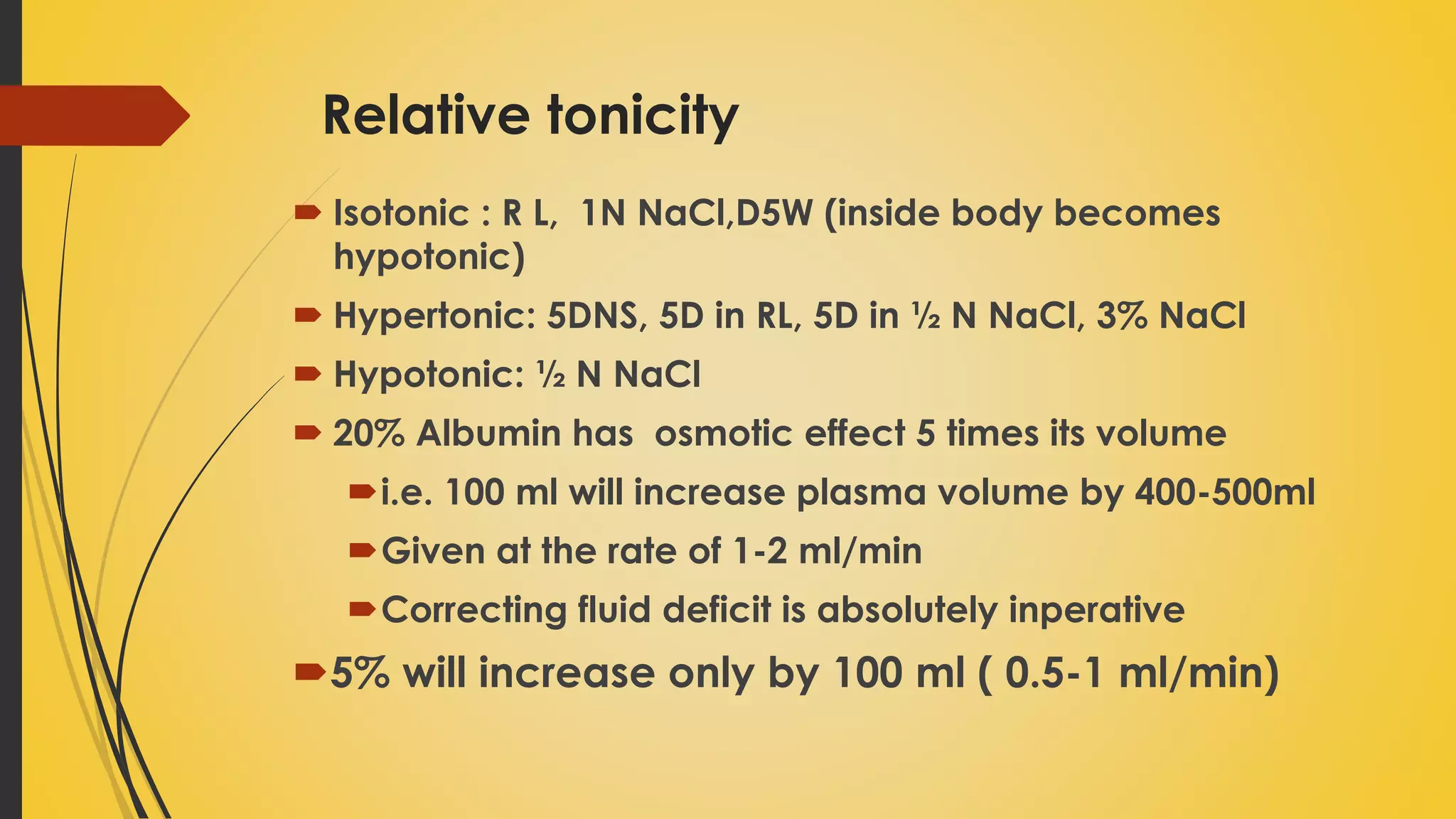
Describes total body water (TBW), its compartments, and percentages in the body, emphasizing ECF and ICF.Explains concepts of osmolality and tonicity including their definitions, measurements, differences, and clinical relevance.
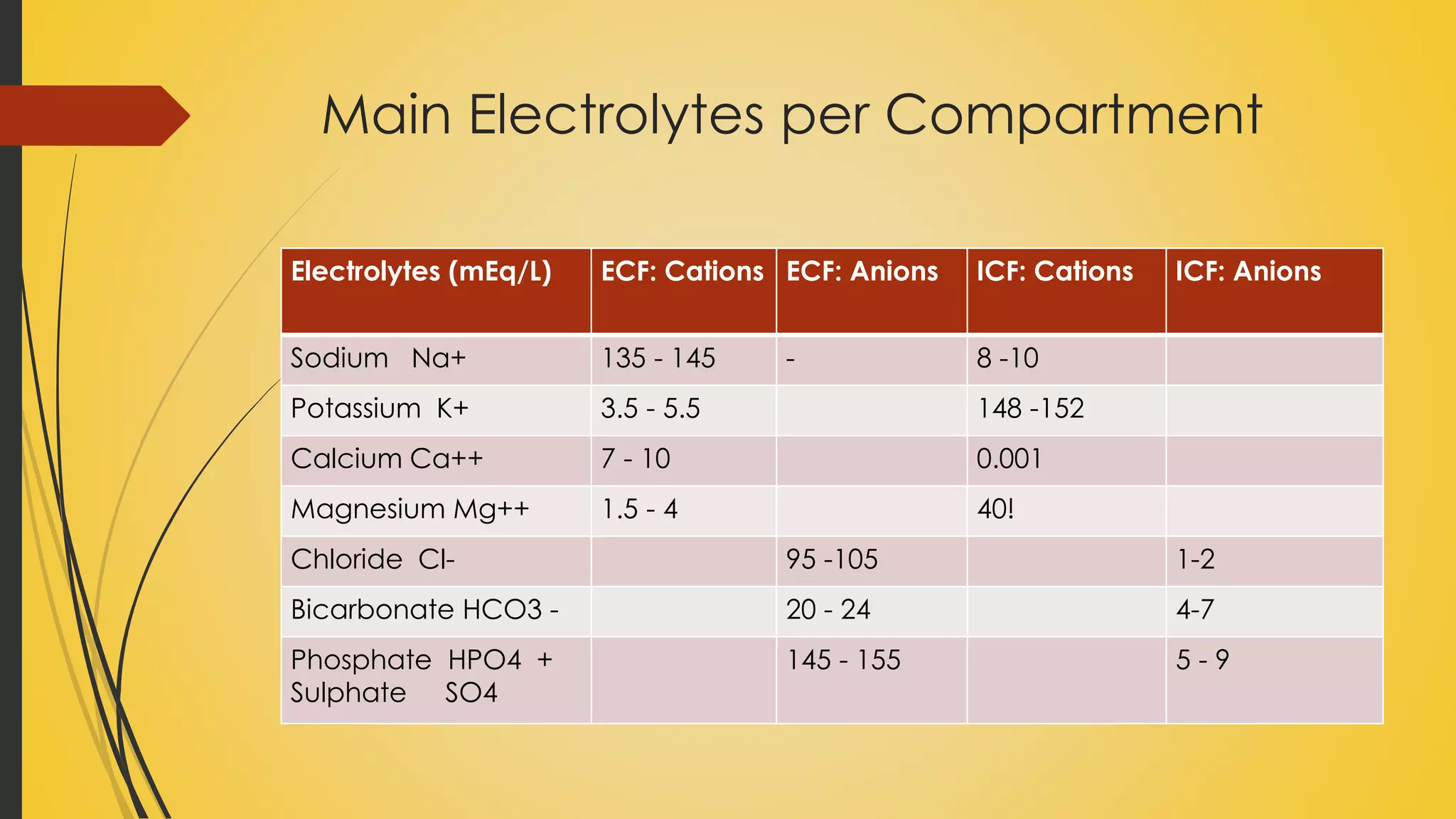
Defines electrolytes, distinguishes between ECF and ICF electrolytes with reference ranges.
Discusses mechanisms of water regulation in the body and insensible water losses including daily requirements.
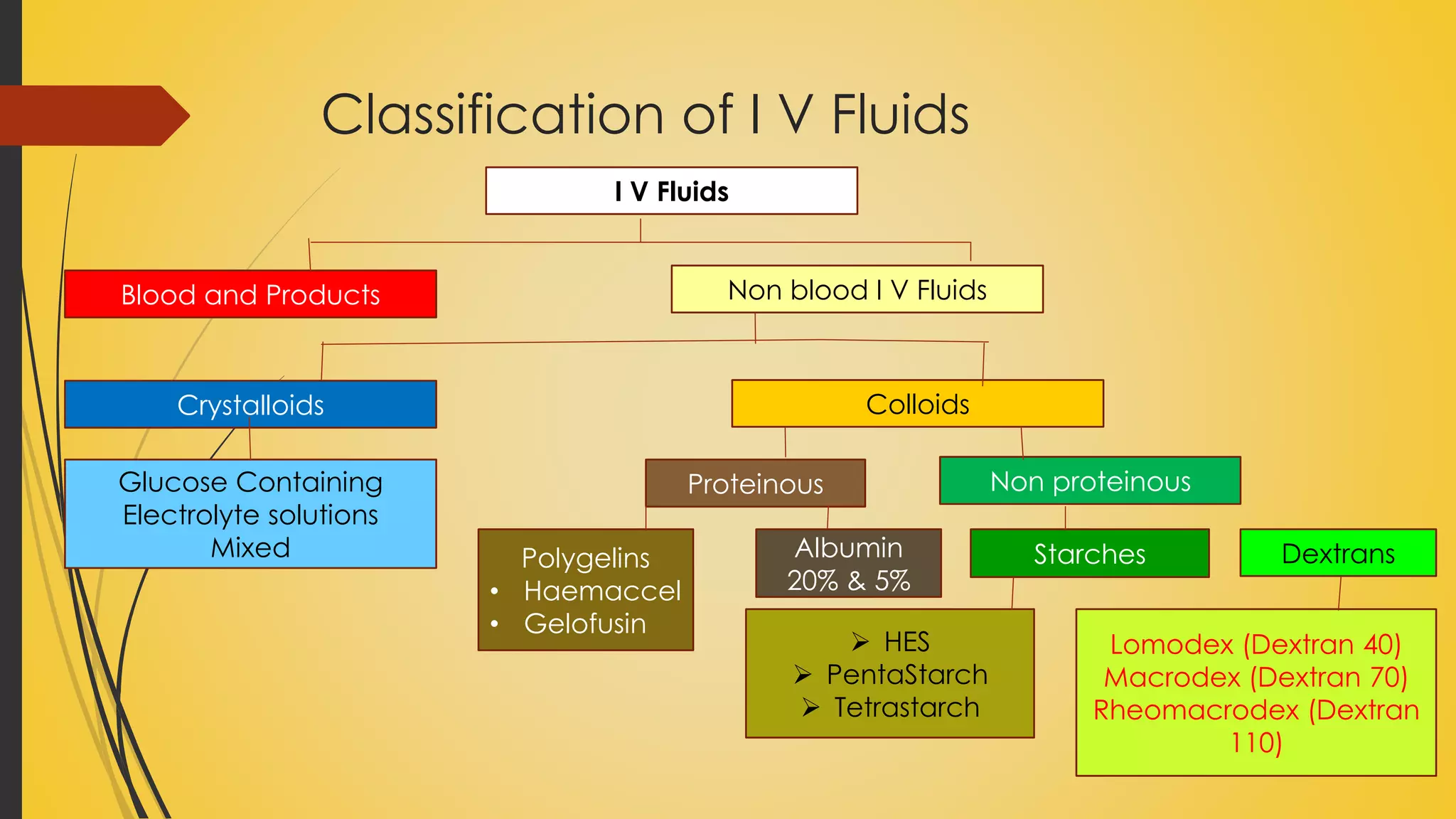
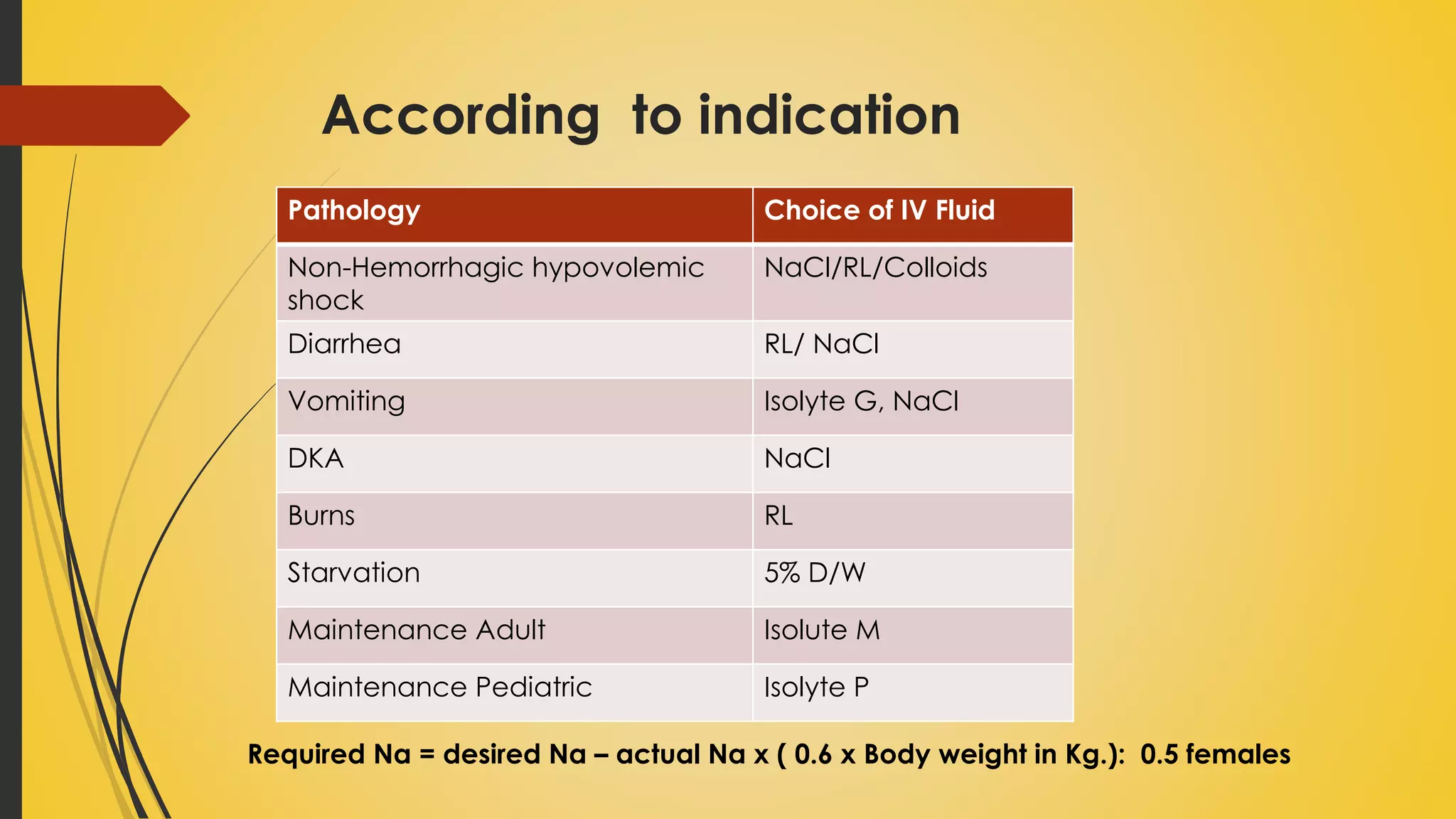
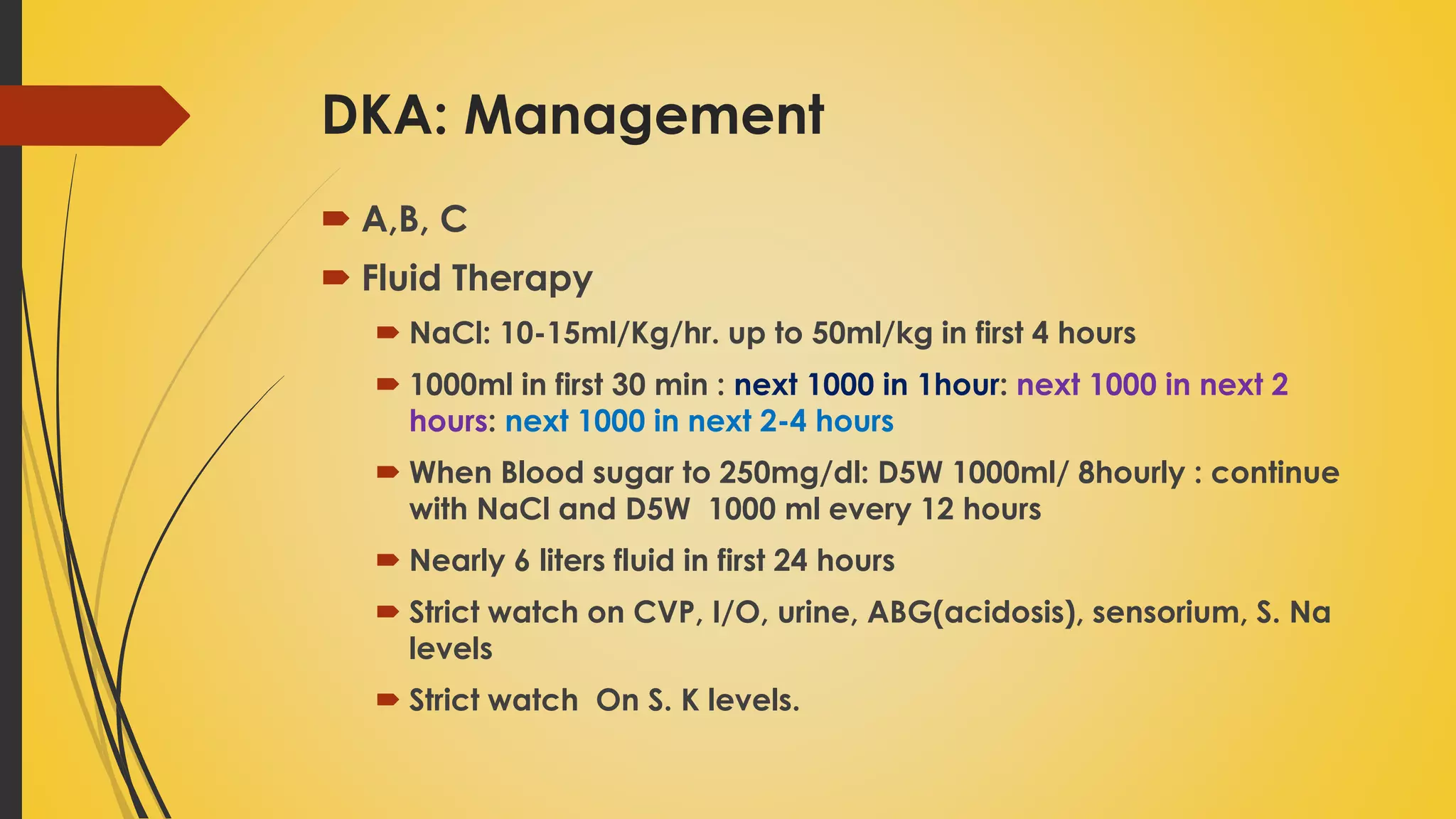
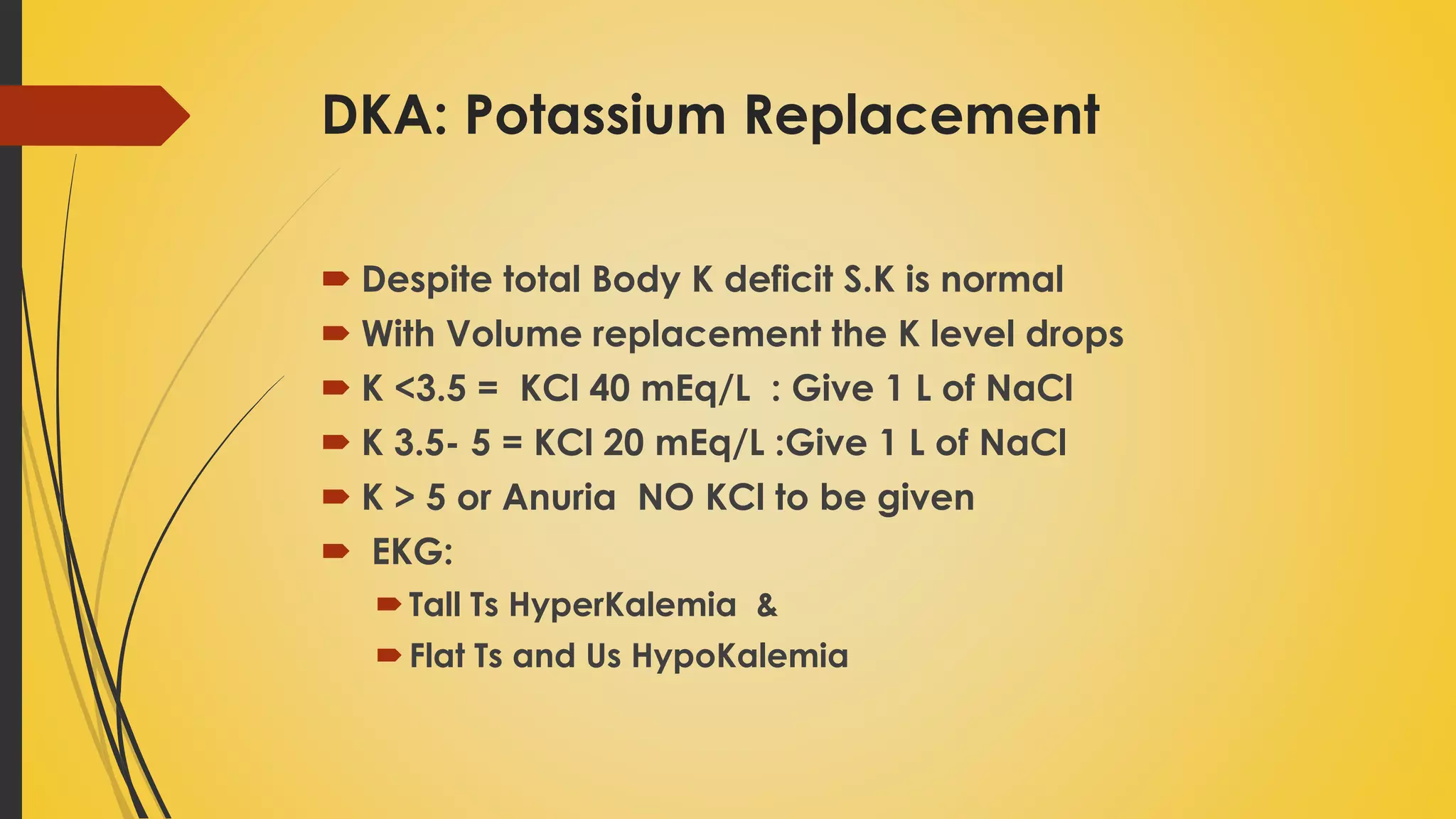
Categorizes IV fluids, corrects hypovolemia, and outlines management for conditions like DKA and SIADH.
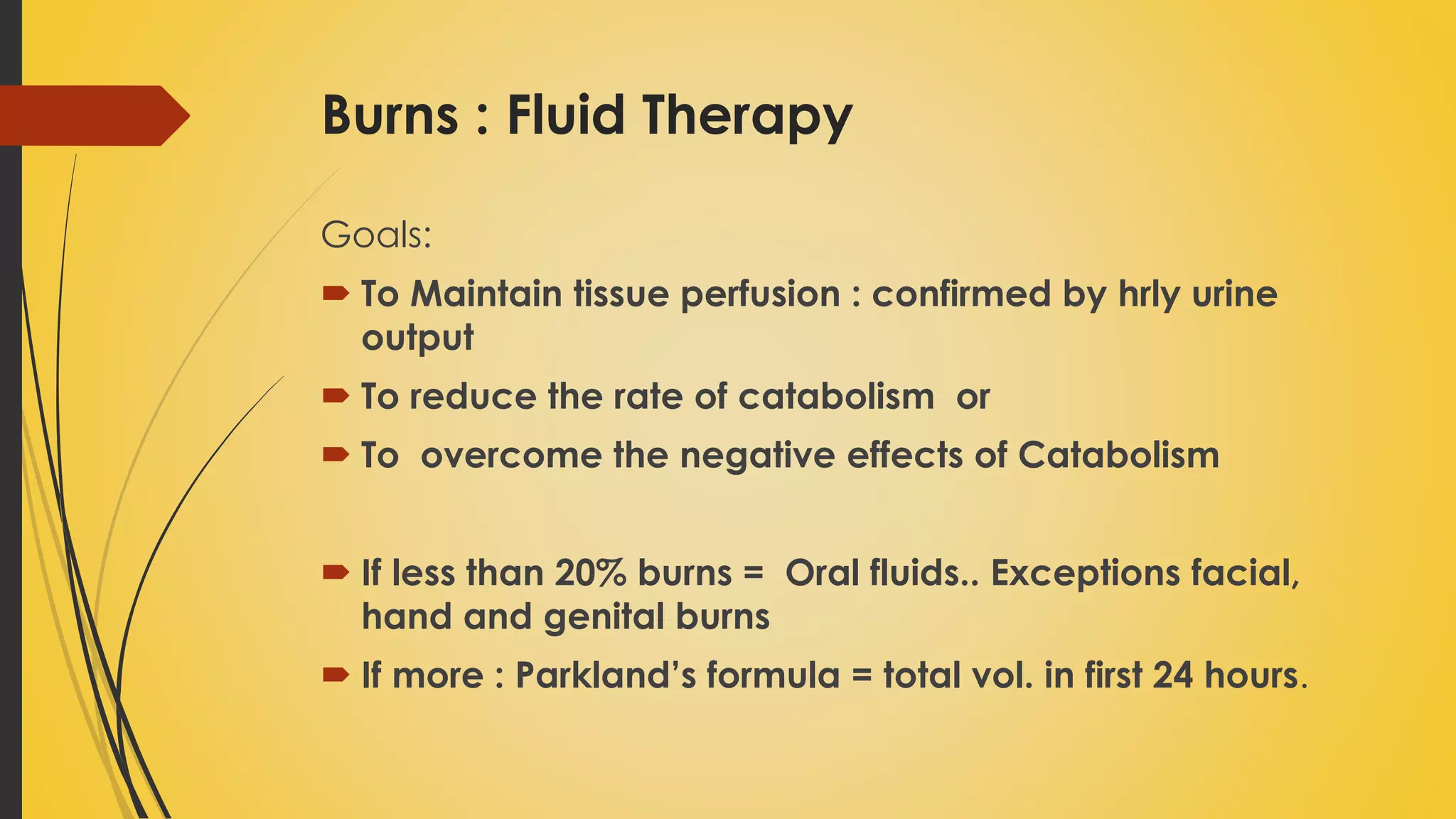
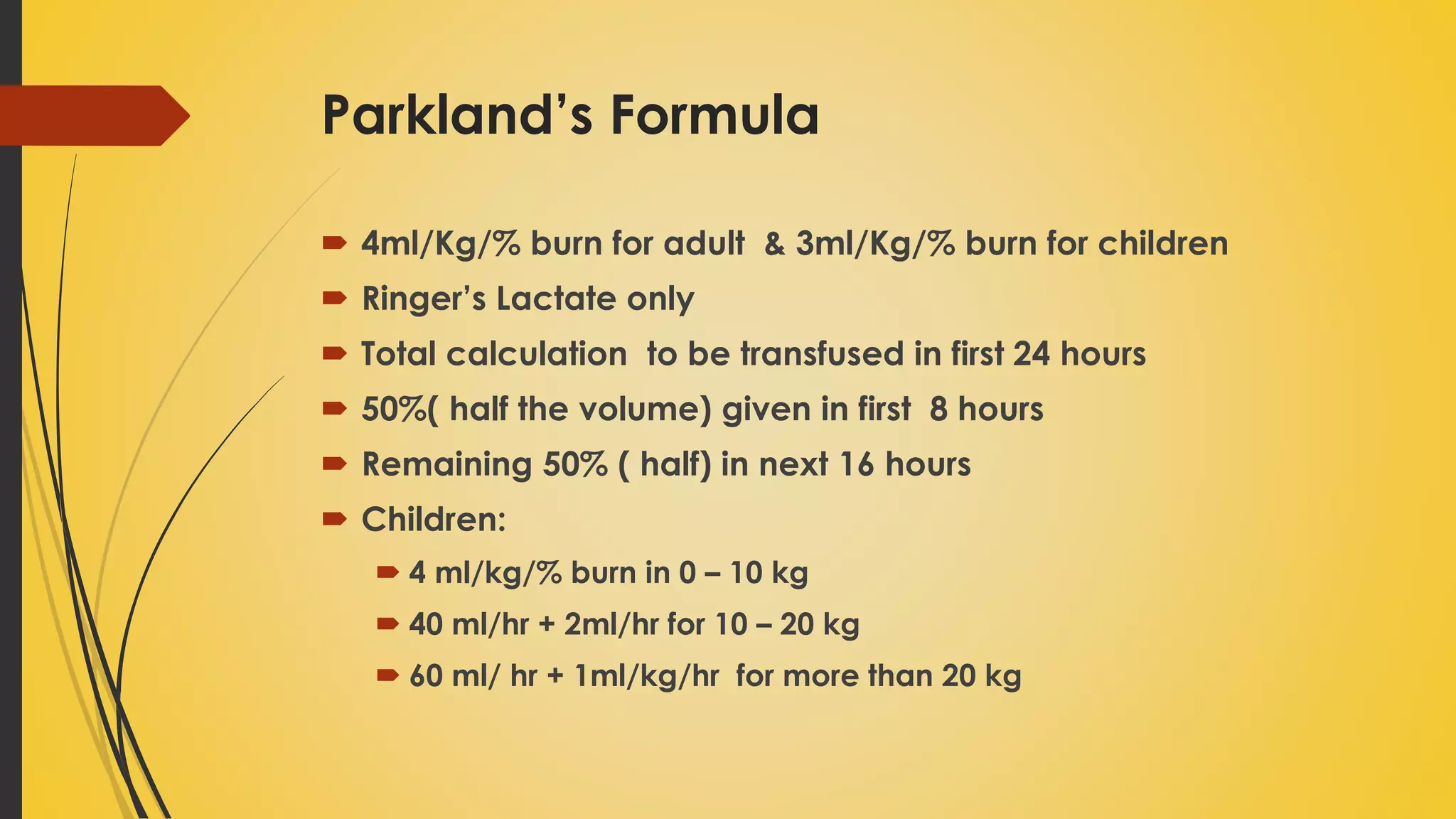
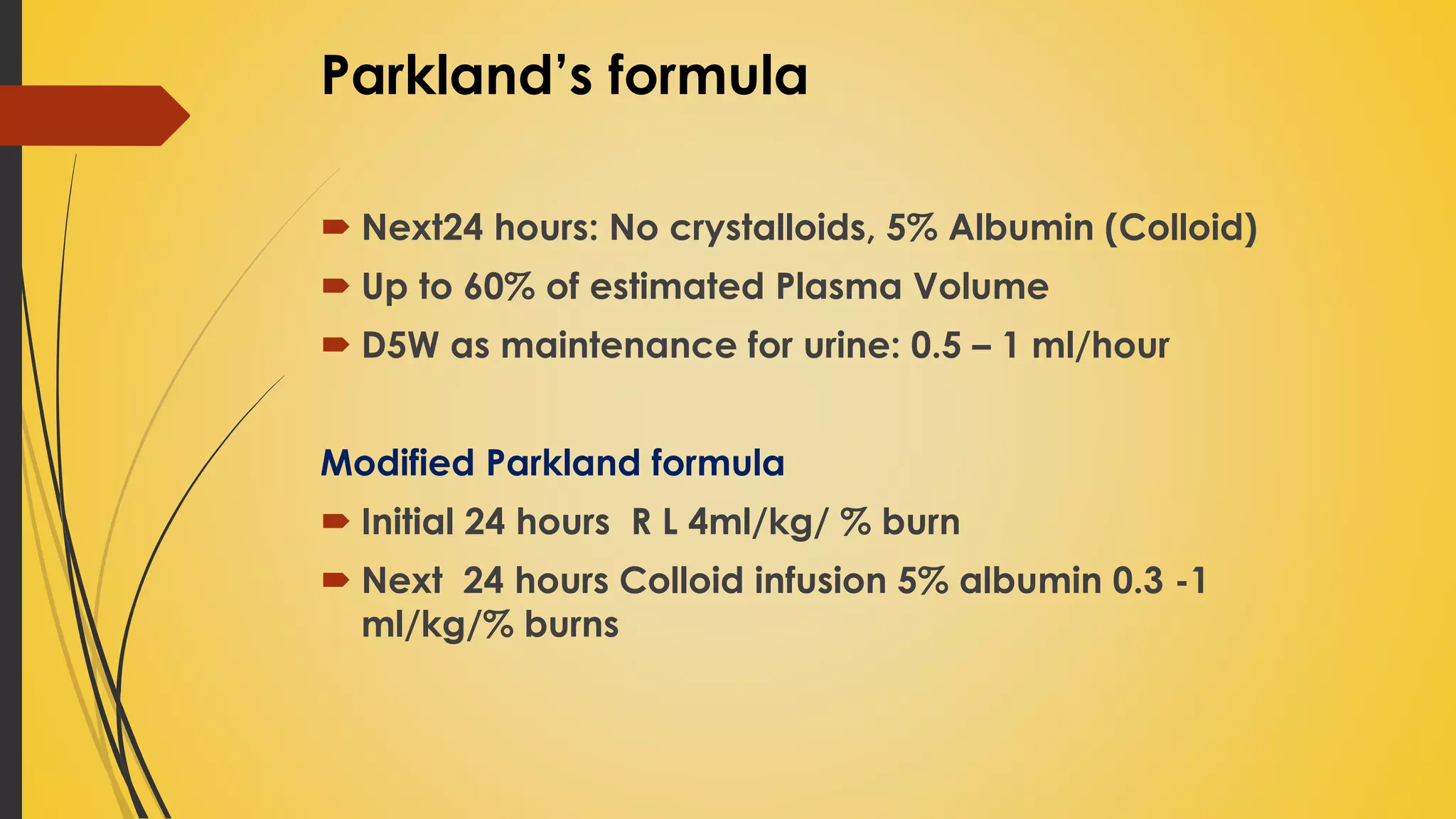
Details fluid therapy goals for burn patients and introduces Parkland's formula for fluid calculation.