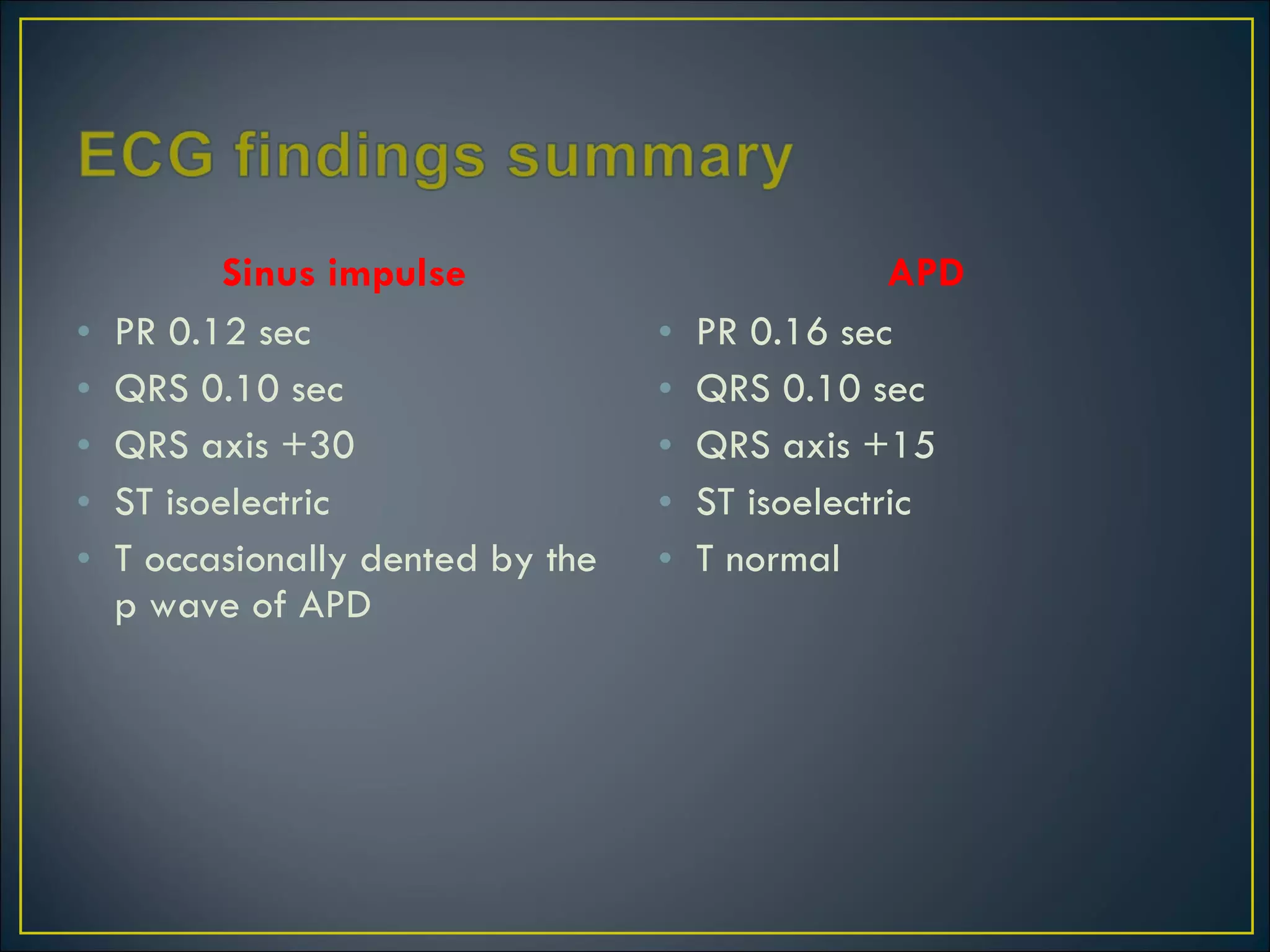
The patient presented with an irregular pulse. An ECG showed evidence of two foci of atrial depolarization, indicating both right and left atrial premature depolarizations (APDs). The ECG pattern is known as atrioventricular bigeminy. The APDs are arising from a single irritable focus in the atria, which can be caused by various stimulants, toxins, or medical conditions. While usually benign, atrial bigeminy can potentially lead to more serious arrhythmias. Management involves correcting any underlying predisposing factors.