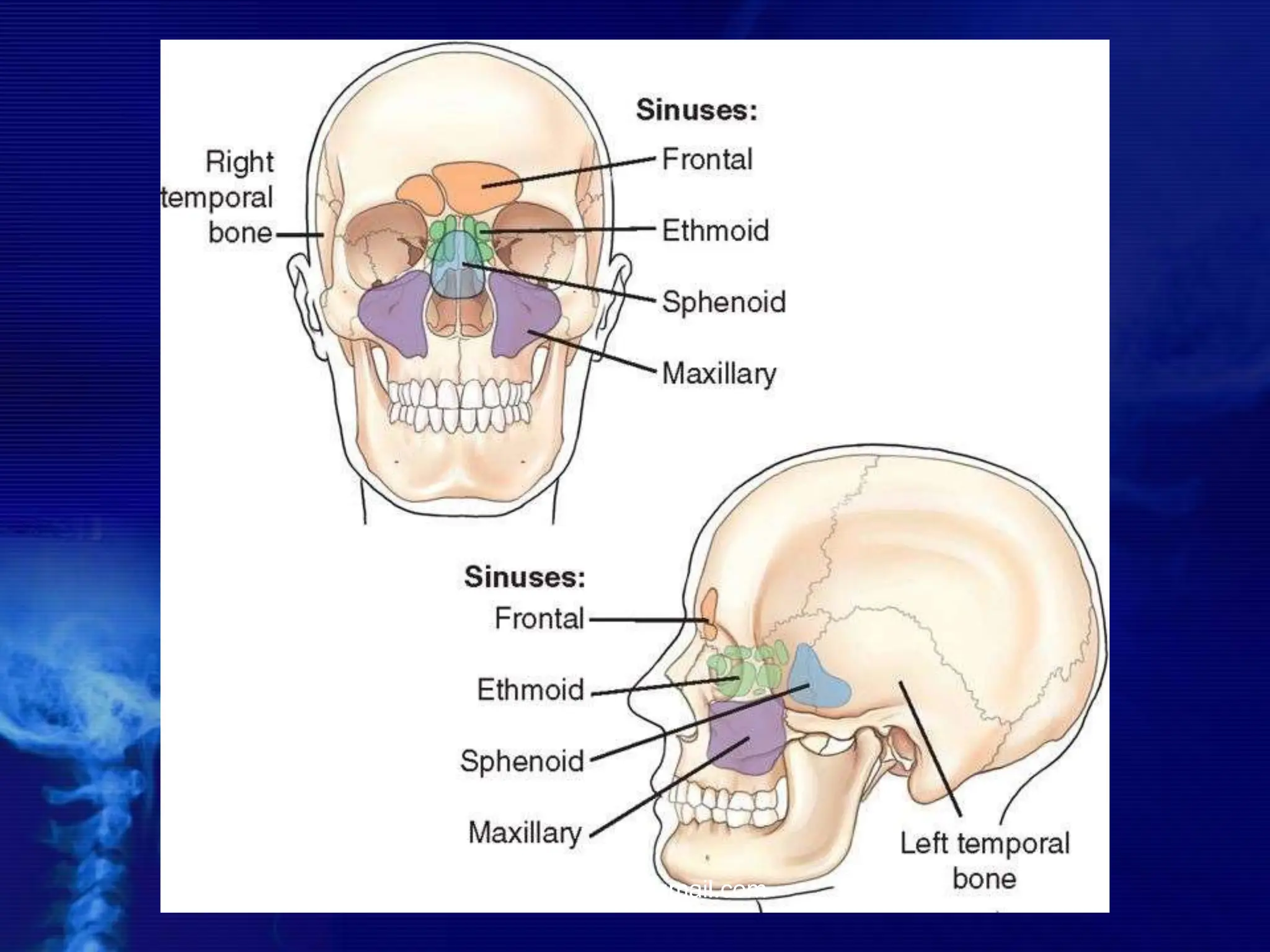
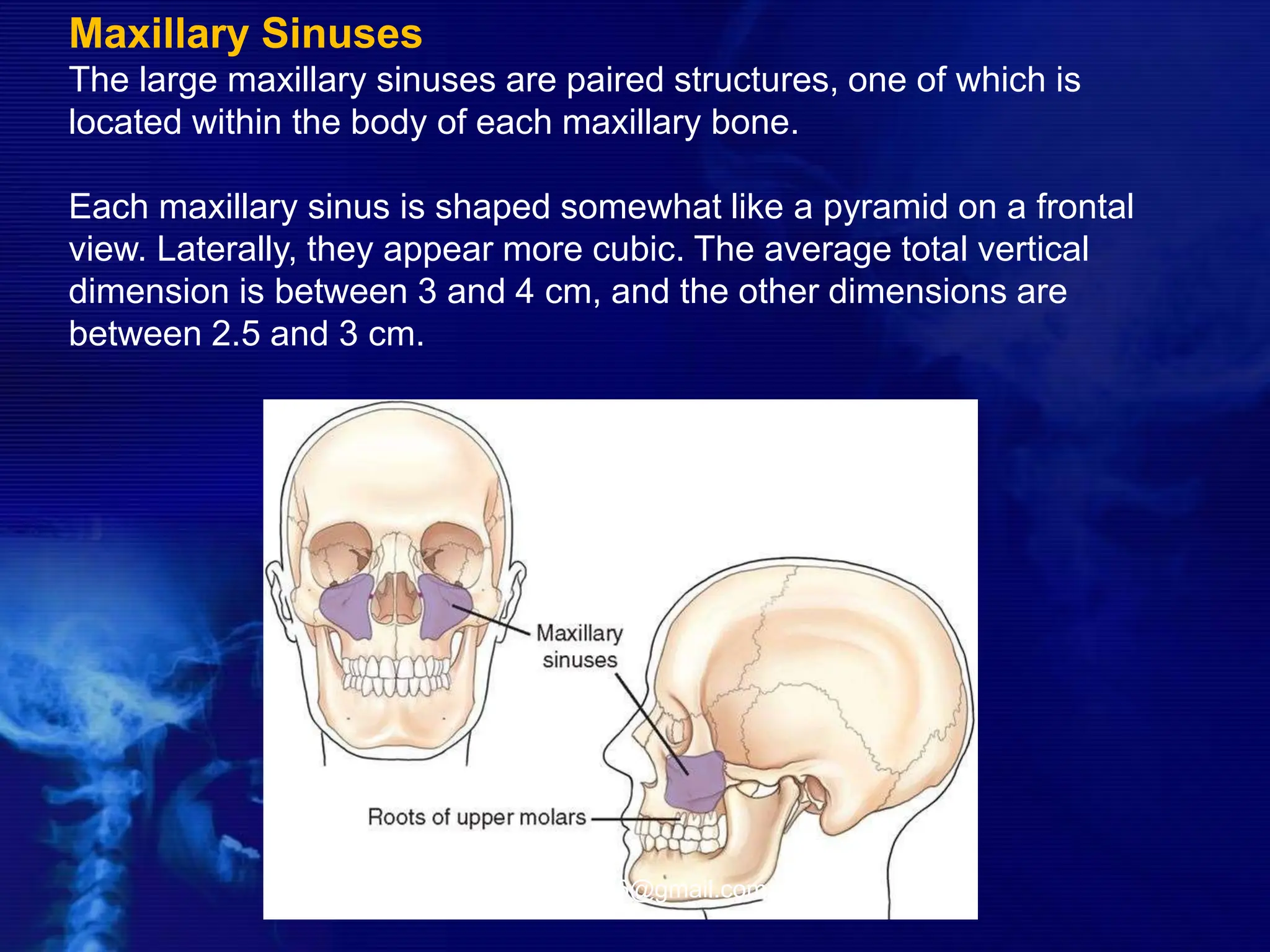
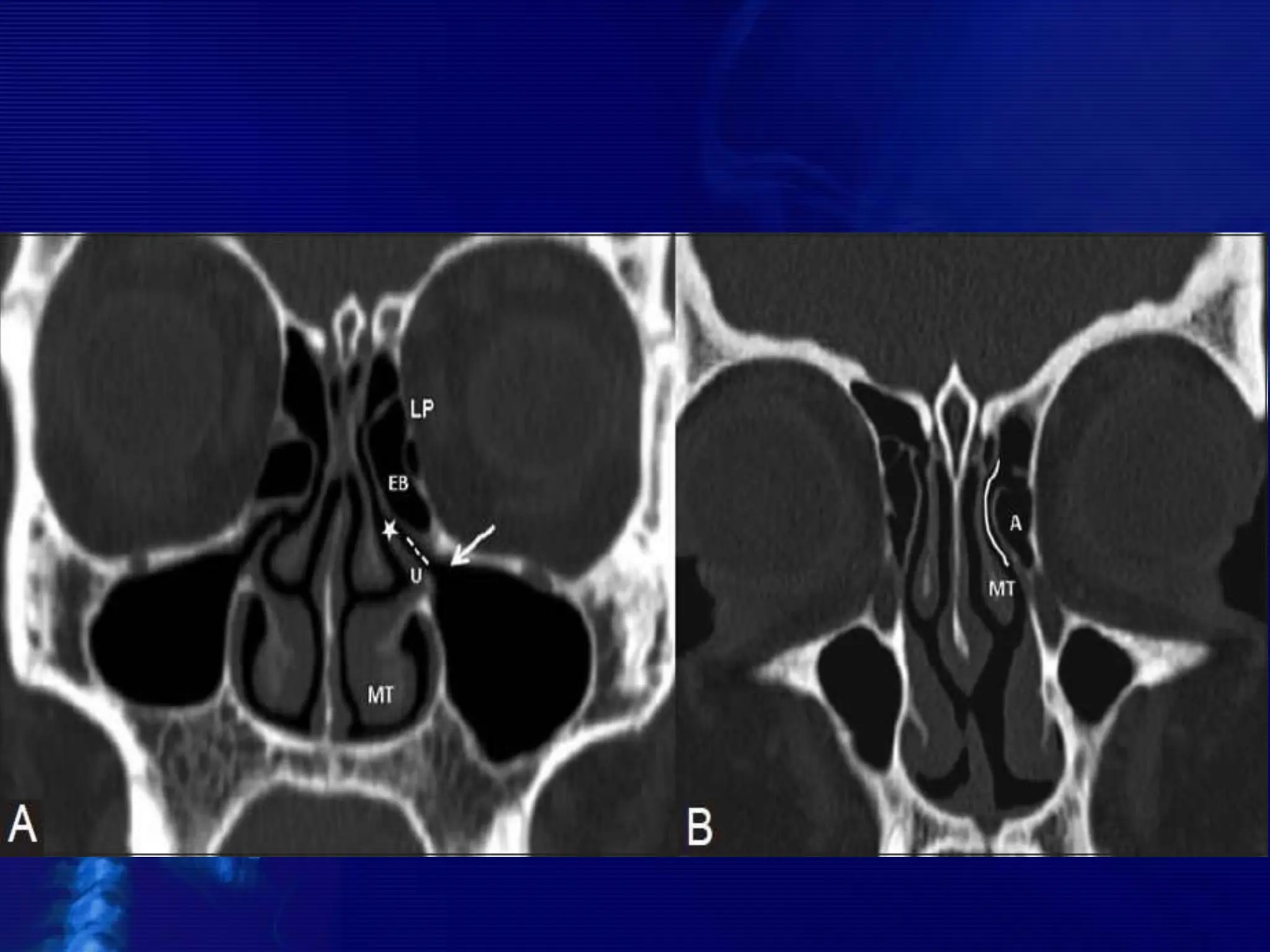
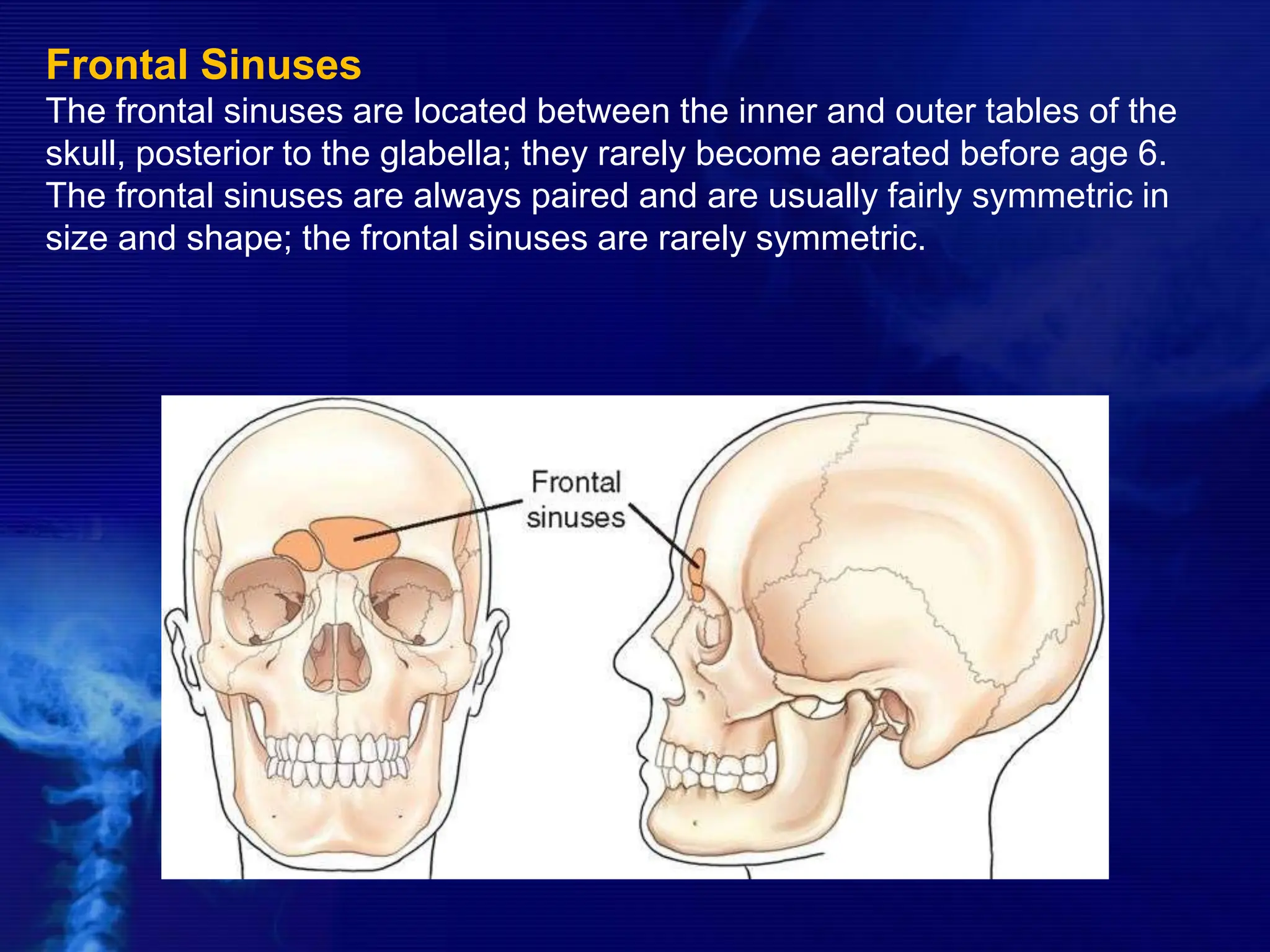
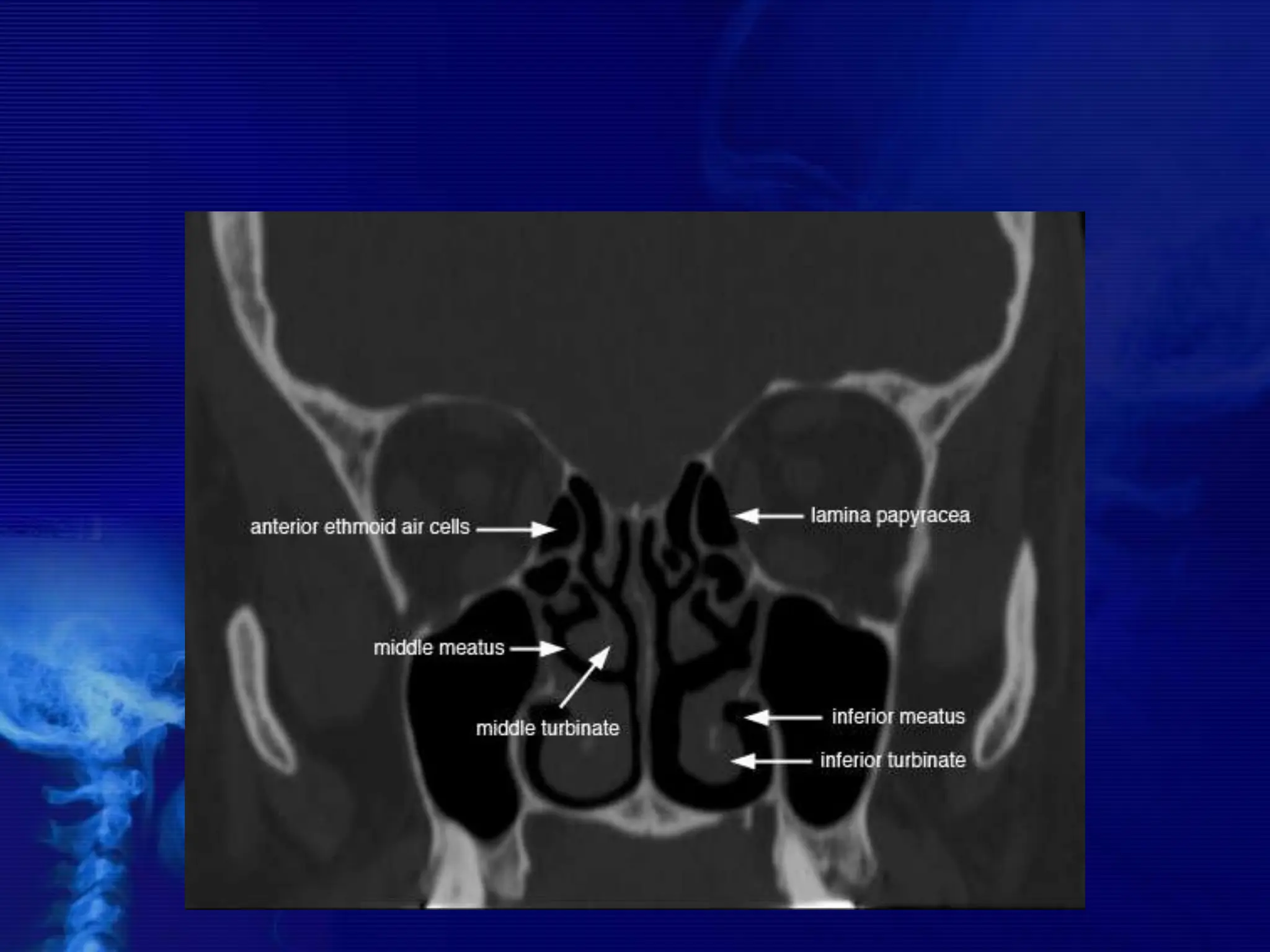
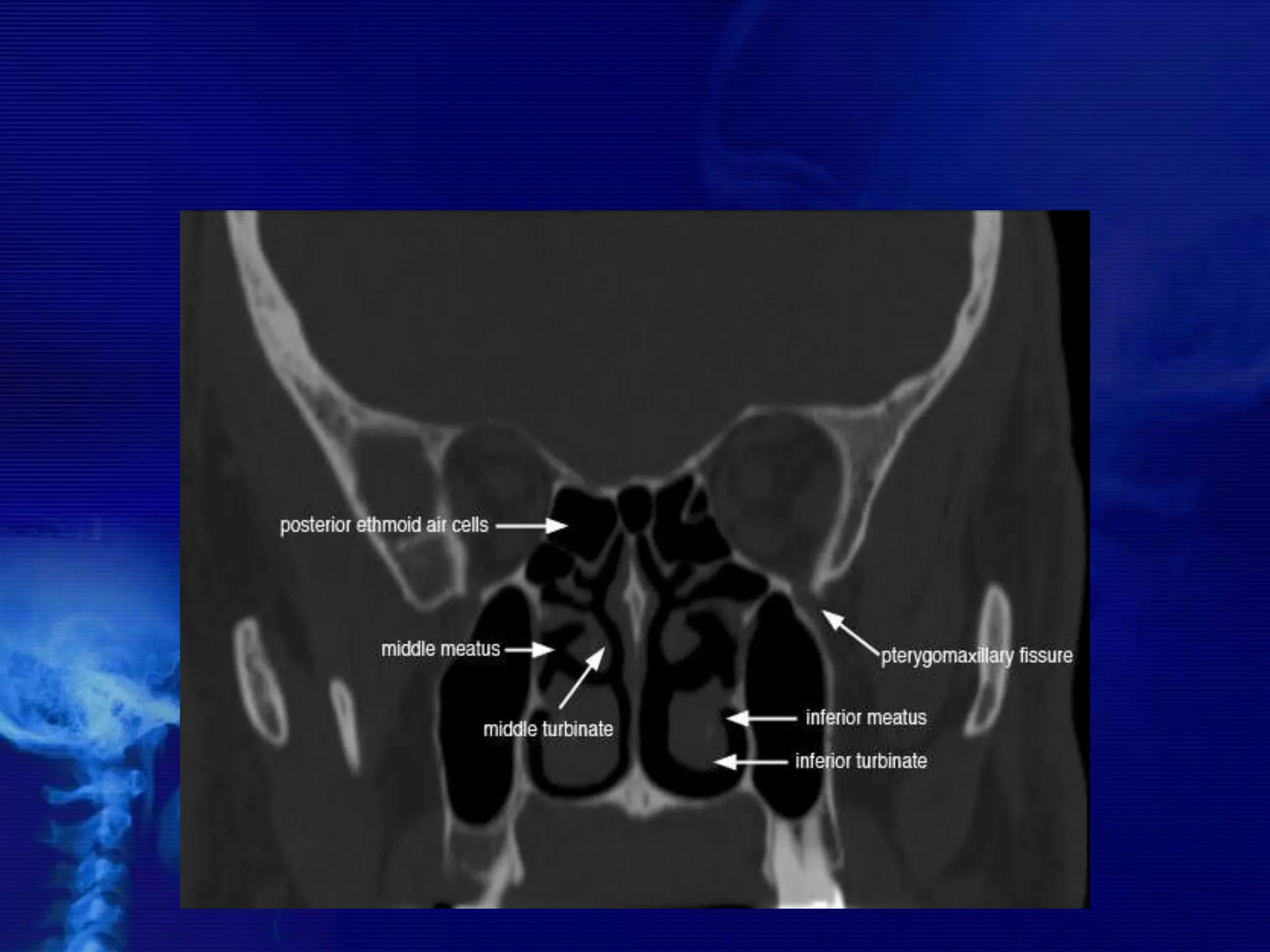
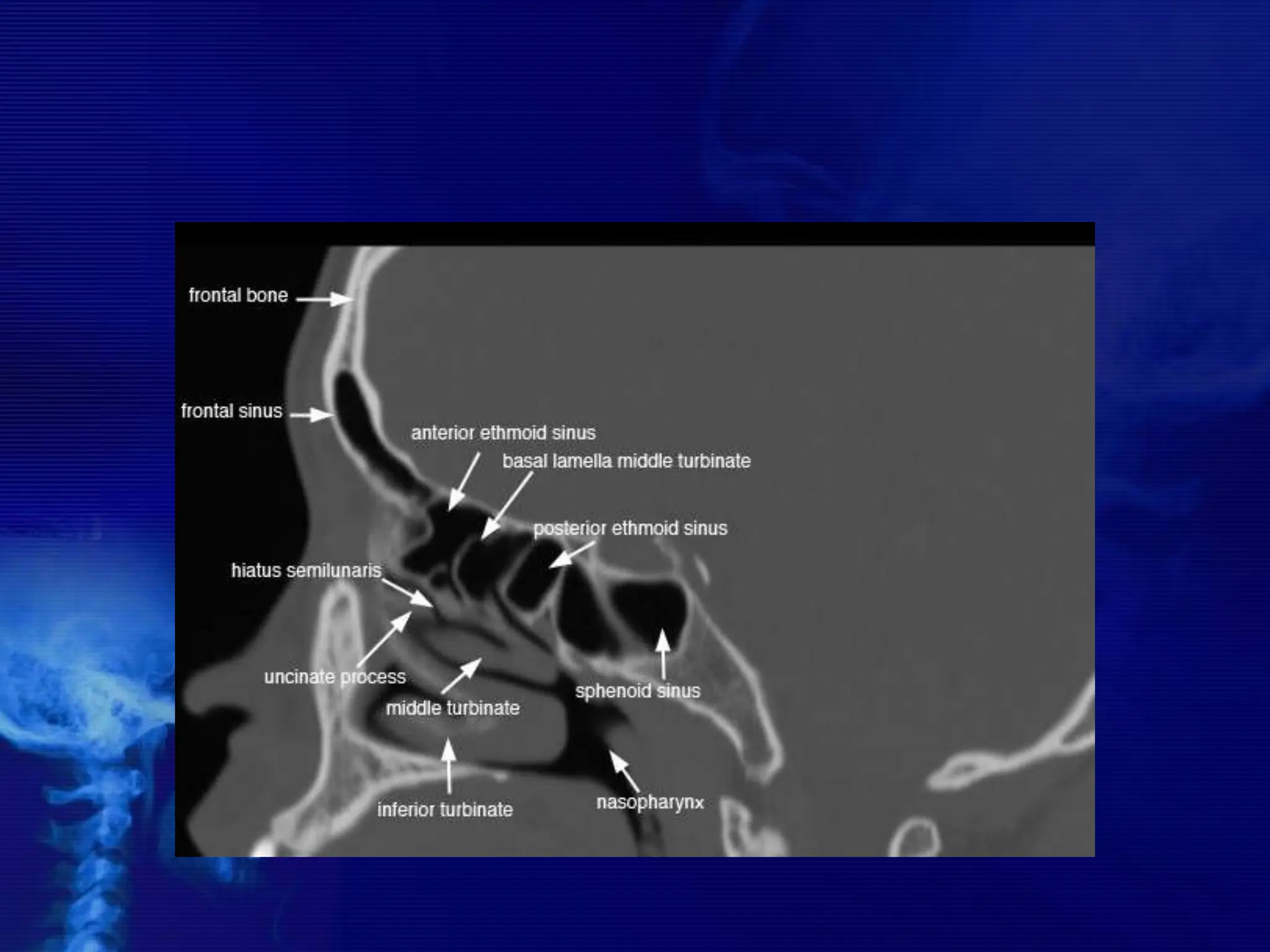
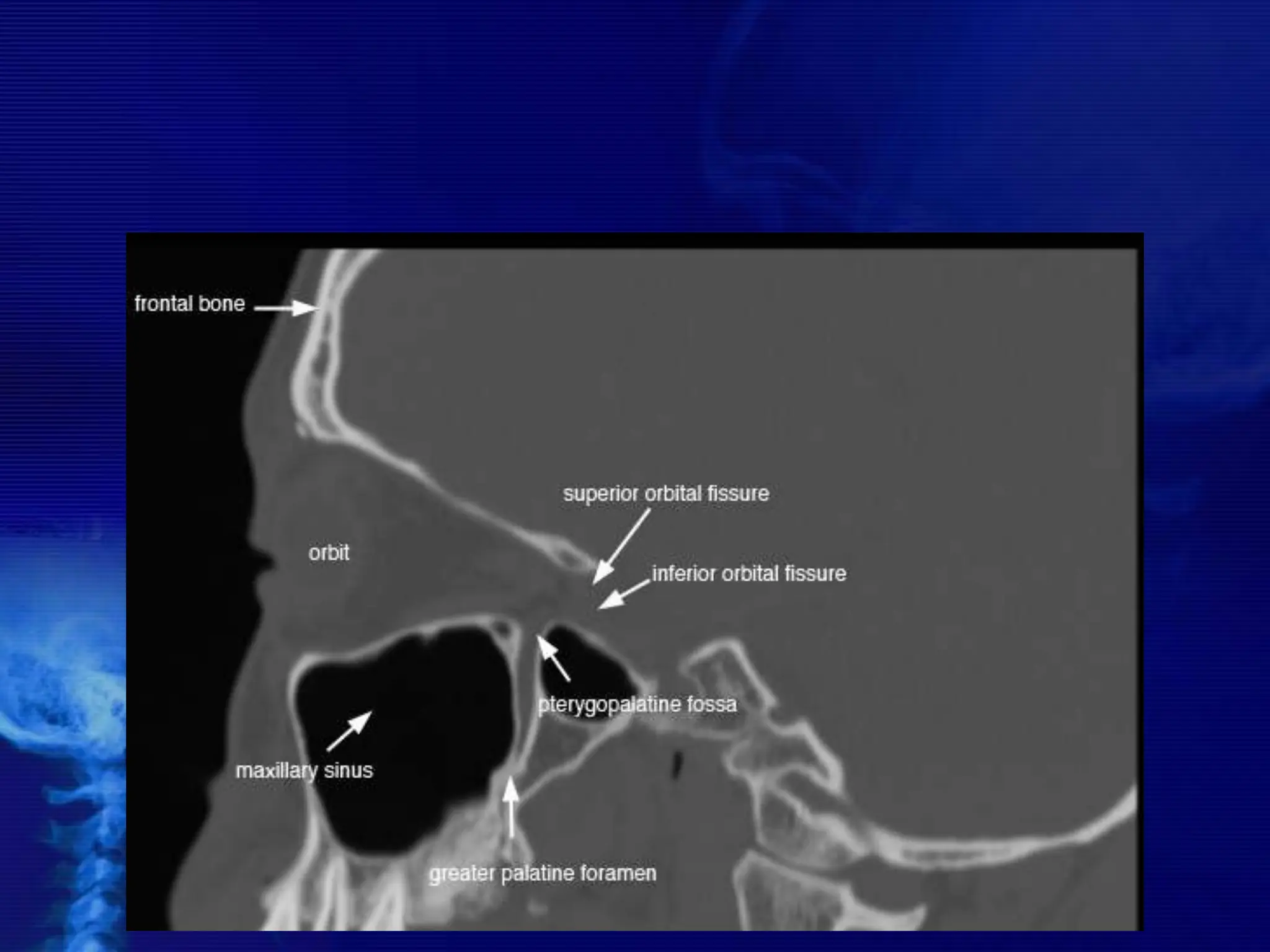
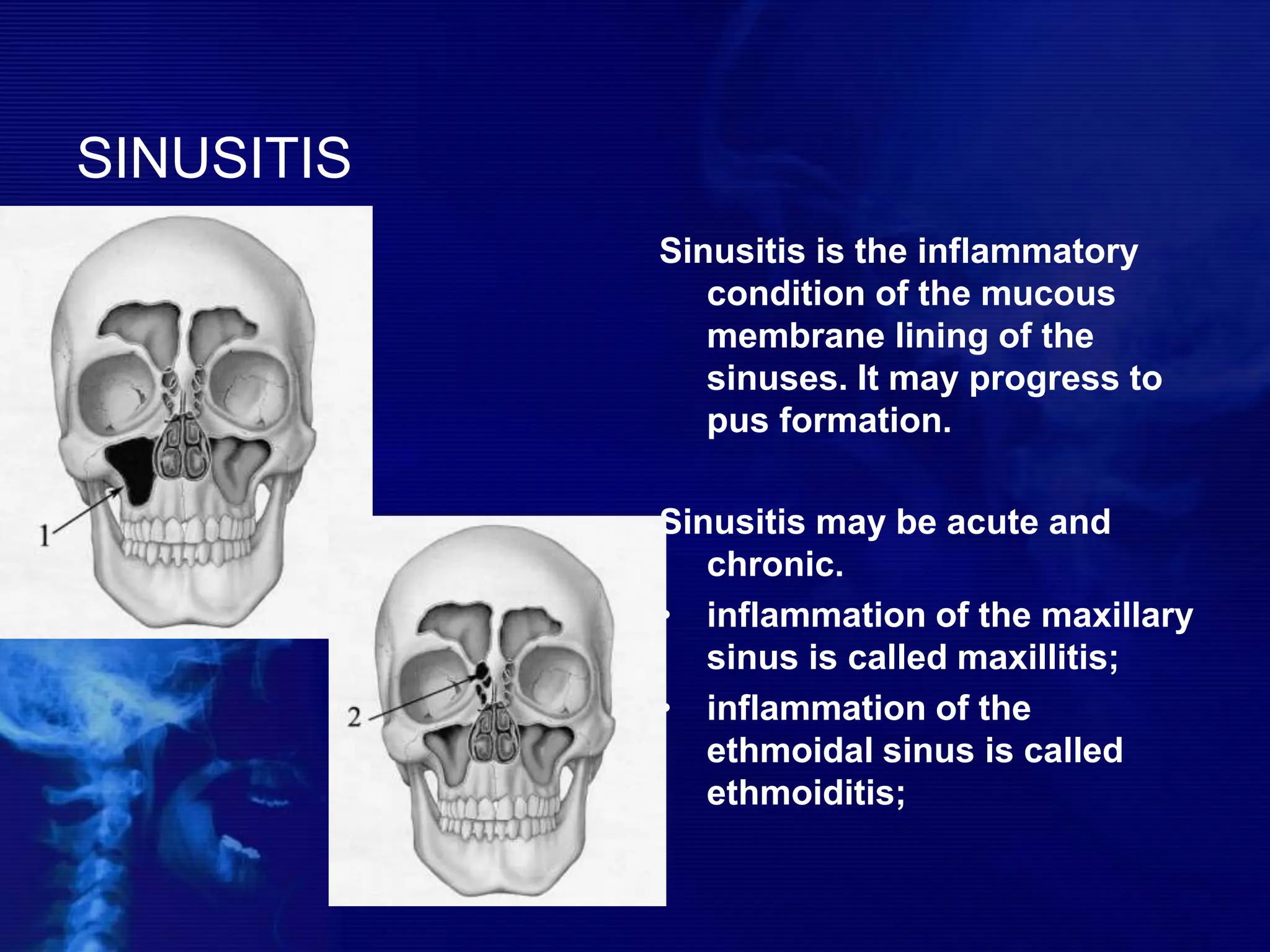
The document provides an overview of the anatomy, pathology, and imaging techniques related to the paranasal sinuses, which include the maxillary, frontal, ethmoid, and sphenoid sinuses. It discusses the function of these sinuses, common conditions such as sinusitis, and the importance of imaging techniques like X-rays and CT scans for diagnosing sinus conditions. Various types of sinusitis, their symptoms, and the pathophysiological processes involved are also elaborated.