Paranasal sinus diseases and their management
•Download as PPTX, PDF•
9 likes•1,286 views

Detailed discussion on tumors and other pathologies of paranasal sinus and their management. Surgical anatomy and approaches are also discussed. Complications of PNS surgeries are discussed briefly

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Paranasal sinus diseases and their management
Similar to Paranasal sinus diseases and their management (20)
More from Dibya Falgoon Sarkar
More from Dibya Falgoon Sarkar (18)
Recently uploaded
Recently uploaded (20)
Paranasal sinus diseases and their management
- 1. Presented by: Dr Dibya Falgoon Sarkar
- 2. Paranasal sinuses • Introduction • Development • Anatomy • Physiology • Examination and investigations Paranasal sinus pathologies • Classification • Description • Complications • Treatment
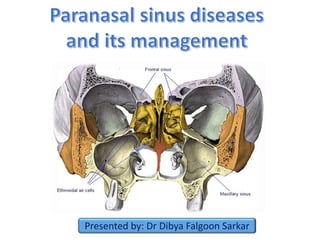
- 3. • Paranasal sinuses are the mucosa lined air spaces present within the bones of the face & skull. • There are four bilaterally paired paranasal sinuses: - Frontal sinus - Maxillary sinus - Ethmoidal sinus - Sphenoidal sinus • Named after the bones in which they are located
- 4. 1. Frontal sinus 2. Ethmoidal sinus 3. Sphenoidal sinus 4. Maxillary sinus
- 5. • Humidifying and warming the inspired air. • Imparts resonance to voice • Increases surface area for absorption of noxious gases and trapping of particles in inspired air •Lightens the skull •Helps in absorbing the shock of blows to the face & thereby limiting the extent of facial injury from trauma. •Serves as an accessory olfactory organ by evenly distributing the inspired air. •Contributes to facial growth
- 6. Sinuses begin their development at the 3rd month of intrauterine life as outpouchings of the mucous membranes of the nasal meatuses and sphenoethmoidal recess The early PNS expand into the walls of the nasal fossa by the growth of mucous membranes into the maxillary, sphenoid, ethmoid and frontal bones Pneumatization follows. Sinuses enlarge variably but always retain their original communication with the nasal cavity through ostia
- 8. • Largest of all the paranasal sinuses. • Also known as the “antrum cave of Highmore”– English physician described an infection of sinus in 1651. • First sinus to develop • Pyramidal shaped - base toward the lateral wall of nose and apex directed laterally into the zygomatic process • Capacity approx. 15ml
- 9. Superior wall • This wall forms both- roof of sinus & floor of the orbit. • It is thinnest wall & mostly flat slopes slightly anteriorly and laterally. • The Infraorbital canal runs along this wall and crosses from back to front- accentuates the fragility of wall • This wall is frequently involved in orbital and maxillary trauma. Anterolateral wall • Thickness is 2-5mm.Thinnest portion over canine fossa • Related to facial artery and vein • Labial levator muscles & inferior portion of orbicularis oculi is attached to this wall above the infra-orbital foramen. • These attachments direct the spread of infection from maxillary teeth. • This wall also contains the anterior & middle superior alveolar nerves. • Any surgical procedure through this wall may jeopardise the nerve supply to these teeth.
- 10. Floor of the maxillary sinus • It is approximately 1.5 cm below the floor of nasal cavity. • It corresponds to the line drawn laterally from ala of the nose. Posterolateral wall • Posterior superior alveolar nerves and vessels sometimes present in close contact with the sinus mucosa. • In such instances , acute sinusitis is accompanied by pain in multiple maxillary posterior teeth. • Immediately posterior to this wall, vital structures include: -maxillary nerve & maxillary artery - nerve of pterygoid canal - sphenopalatine ganglion.
- 11. Ostium of maxillary sinus • Communication between maxillary sinus and nasal cavity. • Average length: 5.5mm • Located superior to the floor of the sinus. • Opens into posterior part of hiatus semilunaris in the middle meatus • Arterial supply: - Facial artery - Infraorbital artery - Greater palatine artery. • Venous drainage: - Facial vein - Infraorbital vein Nerve supply: Infraorbital nerve Anterior , Middle & Posterior superior alveolar nerves Lymphatics: Submandibular lymph nodes
- 12. • The frontal sinuses are rudimentary or absent at birth. • They are developed between 7th & 8th year of life but reach the full size only after puberty. • Situated between the inner and outer tables of frontal bone • Absent on one (15 %) or both sides (5 %) • Drainage pathway – naso- frontal duct- frontal recess - situated at its floor • Drains into middle meatus (62%) or ethmoid infundibulum (38%).
- 13. • The inner table is much thinner than the outer table. As a result the chances of fracture of the inner table are more frequent ,even without the fracture of outer table. Arterial supply: - supraorbital artery - anterior ethmoidal artery Venous drainage: Anastomotic vein in the supraorbital notch connecting the supraorbital & superior ophthalmic veins. Lymphatic drainage: Submandibular nodes. Nerve supply: Supraorbital nerve
- 14. • Formation begins at 4th month of fetal life • Thin-walled air cavities in the lateral masses of ethmoid bone, between nose and the eyes. • Anterior ethmoidal air cells -3- 11 drain into either the ethmoidal infundibulum or the frontonasal duct. • Bullar cells (middle ethmoidal air cells) -usually <3 - open in ethmoidal infundibulum. • Posterior group :- Up to 7 - usually drain by a single orifice into the superior meatus
- 15. Ethmoidal bulla: • This is the most constant landmark for surgery. It lies above the infundibulum and it's lateral/inferior surface and the superior edge of the uncinate process forms the hiatus semilunaris. • The anterior ethmoid artery usually decends across the roof of this cell. Arterial supply: - Sphenopalatine artery - Anterior and posterior ethmoidal arteries Venous drainage: Corresponding veins Lymphatic drainage: • Anterior and middle groups drain in the submandibular nodes . • Posterior group drains into retropharyngeal nodes. Nerve supply: Anterior and posterior ethmoidal nerves Orbital branches of pterygopalatine ganglion.
- 16. • They are the most anterior ethmoidal air cells. • Its size influence the patency of the frontal recess and the anterior middle meatus. • Haller cells: Also called infraorbital ethmoid cells. • Present in approx. 20 % patients. • Clinical significance – 1. Become infected , with potential extension into orbit. 2. Narrows the maxillary ostium. • These are posterior ethmoidal cells extending into the sphenoid bone, either adjacent to or impinging upon the optic nerve. • When these Onodi cells abut or surround the optic nerve, the nerve is at risk when surgical excision of these cells is performed.
- 17. • Body of sphenoid - behind the nose, in the centre of the skull. • Rarely symmetrical and separated by a thin bony septum. • Ostium of the sphenoid sinus is situated in the upper part of its anterior wall and drains into sphenoethmoidal recess. • Average size – 2 x 2 x 2 cm. • According to Congdon sphenoid pneumatization can be as follows: 1. Conchal – 5 % 2. Presellar – 23 % 3. Postsellar – 67% • Arterial supply- Posterior ethmoidal artery. • Nerve supply- Posterior ethmoidal nerves • Lymphatic drainage- Retropharyngeal nodes
- 18. • History and systemic clinical examination: • Check general signs of health • Systemic medical history, history of allergies, drug use and abuse • Occupation history • Examination of neck for lumps or swollen lymph nodes • Palpation: • PNS may be palpated directly to elicit any tenderness • Tenderness over maxillary and frontal bones may indicate inflammatory condition • Step-off deformity indicates facial bone fracture in trauma cases • Paresthesia is seen over midface region in injury to infraorbital nerve
- 19. 1. Anterior rhinoscopy: • Examination of nose with a nasal speculum to check for abnormal areas, useful in evaluation of nasal obstruction. • Colour of nasal mucosa and its vascularity • Position of septum is noted for deviation or dislocation, as well as septal spurs, haematoma or perforations • Inferior & middle turbinates seen 2. Posterior rhinoscopy: • Assessed using a mouth mirror and headlight in the nasopharynx • Technique sensitive
- 20. • Low specificity and sensitivity • Helpful in absence of endoscopy • Decreased light transmission when compared with normal side suggests of significant fluid collection or marked mucosal edema Transillumination
- 21. • Endoscopic examination/ Rhinoscopy: Nasoscope/rhinoscope is a thin, tube-like instrument with a light and a lens for viewing. • A special tool on the nasoscope may be used to remove samples of tissue. The tissues samples are viewed under a microscope by a pathologist. • Helps in visualization of inaccessible areas like middle meatal cleft.
- 22. 1. Maxillary sinus: • Water’s view (PNS view) x-ray and CT scan are ideal for maxillary sinus visualization. • X-ray beam angled at 45 degree to orbitomeatal line 2. Frontal sinus: • CT scan is helpful in trauma cases as we can appreciate both inner and outer tables in the axial view • PNS view x-ray is helpful to detect fluid accumulation in sinusitis cases 3. Ethmoidal sinus: Axial views of CT scan are helpful in detecting fractures of the ethmoid bone. 4. Sphenoid sinus: Best viewed in sagittal and axial sections of CT scan. “Limited CT Evaluation” – slice 3-4 mm
- 23. Maxillary sinus & Ethmoid air sinus Axial CT scans
- 24. Frontal sinus CT scan axial PNS view radiograph
- 25. Sphenoid sinus Axial CT Sagittal CT
- 26. • MRI: Excellent soft tissue definition - evaluation of neoplastic disease. • MRI (magnetic resonance imaging) with gadolinium: Gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture.
- 27. • Developmental variations and anomalies • Inflammatory/infectious diseases • Cysts • Tumours – benign & malignant • Other surgically relevant conditions
- 28. • Paradoxical curvature of middle turbinate: • Normally the convexity of the middle turbinate is directed medially toward the nasal septum. • When the convexity is directed laterally, it is termed a paradoxical middle turbinate . • Most authors agree that the paradoxical middle turbinate can be a contributing factor to sinusitis.
- 29. • Variation of the ethmoidal roof anatomy • The ethmoid roof is of critical importance for two reasons: 1. most vulnerable to iatrogenic cerebrospinal fluid leaks. 2. anterior ethmoid artery is vulnerable to injury. • The depth of the olfactory fossa is determined by the height of the lateral lamella of the cribriform plate. • In 1962, Keros classified the depth of the olfactory fossa into three types, that is, a) Keros type I: <3 mm b) Keros type II: 4-7 mm c) Keros type III: 8-16 mm - most vulnerable to iatrogenic injury.
- 30. • Variations of uncinate process • The uncinate process may be medialized, lateralized, or pneumatized/bent. • Medialization occurs with giant bulla ethmoidalis. • Lateralization of the uncinate process may obstruct the infundibulum. • Pneumatization (uncinate bulla) can rarely cause obstruction of the infundibulum.
- 31. • Sinusitis is the inflammatory condition of the mucous membrane lining of the sinuses. It may progress to pus formation. • Causes : • Rhinogenous – infection spreads from the nasal cavity. It is the most common way for infection and such sinusitis is the complication of the flu. • Odontogenic – infection spreads from upper teeth. This way is typical only for maxillary sinus. The pathologic process may spreads from upper 4,5,6 teeth apex to the inferior wall of the maxillary sinus • Traumatic • Hematogenic • Allergic
- 32. 1. Initial phase: reversible 2. Ostium obstruction phase 3. Bacterial phase 4. Chronic phase Osteomeatal complex obstruction Decreased ventilation of the sinuses Decreased drainage of the sinuses pO2 decrease, pCO2 increase, mucous stasis Inflammation and viscous mucous, ciliary movement slowing Ciliary damage along with increase in number of anaerobic organisms
- 33. • According to duration: 1. Acute : infection lasting 4 weeks, symptoms resolve completely resolved in < 30 days. 2. Subacute :infection lasting between 4 to 12 weeks, yet resolves completely. 3. Recurrent: ≥ 4 discrete acute episodes per year, each completely resolved in < 30 days but recurring in cycles, with at least 10 days between complete resolution of symptoms and initiation of a new episode 4. Chronic: symptoms lasting more than 12 weeks.
- 34. • According to pathogen: 1. Bacterial: Hospital-acquired acute infections are more often bacterial, typically involving Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa 2. Viral: In immunocompetent patients - in the community is almost always viral (eg, rhinovirus, influenza, parainfluenza). antibiotics given for: • Mild to moderate sinus symptoms persisting for ≥ 10 days • Severe symptoms (eg, fever ≥ 39°, severe pain) for ≥ 3 to 4 days • Worsening sinus symptoms after initially improving from a typical • viral URI ("double sickening" or biphasic illness)
- 35. 3. Fungal: Usually seen in immunocompromised patients because of poorly controlled diabetes, neutropenia, or HIV infection. It is clinically of 2 types: A)Non-invasive fungal sinusitis: • Saprophytic fungal infestation/colonization • Allergic fungal rhinosinusitis (AFRS) • Saprophytic fungus balls (mycetoma) B)Invasive fungal sinusitis – • Chronic invasive fungal sinusitis • Granulomatous invasive fungal sinusitis • Acute (fulminant) invasive fungal sinusitis
- 36. • Risk factors: 1. Obstruction to drainage: most important 2. Defect of self-cleaning mechanism of the mucous membrane of sinus – infections causing immobility of the cilia, Increased viscosity of secretions, Immotile cilia syndrome, Prolonged exposure to cigarette smoke 3. Medications: First generation antihistamines (non sedating do not affect), Anticholinergics, Aspirin, Anesthetic agents, Benzodiazepines 4. Immunodeficiency: Immunoglobulin deficiency (IgA, IgG), diabetes, HIV infection 5. Other factors: prolonged ICU stays, severe burns, cystic fibrosis, and ciliary dyskinesia. According to number of sinuses involved: Hemisinusitis - all sinuses on one side Polysinusitis - several sinuses, but not all, are involved Pansinusitis - all, are involved
- 37. 1.Nasal congestion and discharge 2. Sore throat and postnasal drip 3. Pain or pressure. 4. Oedema of facial tissues. 5. Bad breath or loss of smell (hyposmia/anosmia). 6. Systemic symptoms: Malaise may be present. Fever and chills suggest an extension of the infection beyond the sinuses, rise in temperature, bad appetite, sleep disturbances, changes of the blood (leukocytosis), Productive cough (especially at night) 7. Complications – ocular, neurological, local
- 38. • Diagnosis is mainly clinical • CT scan and cultures - mainly for chronic, refractory, or atypical cases. • Clinical diagnostic criteria include a) 2 major factors b) 1 major and 2 minor factors or presence of pus in nasal cavity. Major factors Minor factors Facial pain/pressure Headache Facial congestion/fullness Maxillary dental pain Nasal drainage/discharge Halitosis Postnasal drip Cough Fever (acute sinusitis only) Purulence in nasal cavity on examination Hyposmia
- 39. Treatment options measures to enhance drainage: 1. Heat therapy: Steam inhalation and hot beverages 2. Topical vasoconstrictors/ Nasal decongestants: Topical nasal sprays (limit use to 3-7 days) - Phenylephrine, Oxymetazoline. Corticosteroids: Corticosteroid nasal sprays can help relieve symptoms but typically take at least 10 days to be effective 3. Systemic vasoconstrictors: Systemic vasoconstrictors, such as pseudoephedrine 30 mg 4. Nasal irrigation 5. Antihistaminics: recommended if allergy present. 6. Hydration 7. Antibiotics: Amoxicillin 500 mg tid for 10-14 days - First line Nasal irrigation
- 40. 8. Mucoactive drugs: main purpose - increase the ability to expectorate sputum and/or decrease mucus hypersecretion. 1. Expectorants: hypertonic saline, iodine containing compounds, guaifenesin 2. Mucoregulators: anticholinergic drugs, glucocorticoids, macrolide antibiotics 3. Mucolytics: classic mucolytic (N-Acetyl Cysteine), peptide mucolytic 4. Mucokinetics: bronchodilators, ambroxol a) Nebulization: best form of physiotherapy. b) Laser therapy: used directly over the sinuses to reduce inflammation c) Ultrasound therapy: sound waves are conducted through a hypoallergenic gel to reduce inflammation and loosen the accumulated mucous. d) Short-wave diathermy e) Rinoflow therapy: new option, basically micronized endotracheal wash. Used in sinusitis, rhinitis, pharyngitis, laryngitis and secretory otitis media.
- 41. Indications: • Sinusitis unresponsive to antibiotic therapy • Necrotic sinusitis • Orbital complications (abscess and phlegmon of orbit) • Intracranial complications (meningitis, brain abscess) • Rhinogenic sepsis • Odontogenic sinusitis combined with maxillary osteomyelitis. Approaches: 1. Removal of etiology (eg: removal of the infected teeth) 2. Functional endoscopic sinus surgery (FESS) is the mainstay in the surgical treatment of sinusitis and nasal polyps, including bacterial, fungal, recurrent acute, and chronic sinus problems. 3. Caldwell-luc procedure/ Denker’s procedure 4. Intranasal antrostomy 5. Radical surgeries
- 42. • Oro-antral communication: it is an abnormal connection between oral and Antral cavities. • Oro-antral fistula: long standing oro-antral communication when left open, epithelializes to form a patent fistula between the two cavities. • Types: 1. Alveolosinusal 2. Palato-sinusal 3. Vestibulo-sinusal • Causes: • Extraction – maxillary posterior teeth • Cysts, tumors • Osteomyelitis • Radiation therapy • Trauma • Implant denture Oro-antral Fistula
- 43. • Some patients are asymptomatic • Unpleasant tasting discharge and odor • Reflux of fluids and foods into the nose from mouth • Difficulty in smoking and blowing air • Development of chronic sinusitis in infected cases • Valsalva manoeuvre • Mirror fog test • Cotton wisp test • Nasal regurgitation of fluid • Radiographs: Sinus floor discontinuity, sinus opacity, focal alveolar atrophy.
- 44. Immediate treatment: Primary purpose is closure of defect and prevention of sinusitis through: • Suturing across the defect with/without periodontal pack, warm saline rinses, antibiotic and antihistaminic therapy with decongestants. • Depending on defect size: 1. Size < 5mm: non-invasive intervention (spontaneous closure by blood clot) 2. Size 2-6mm: Collagen plug in the socket with figure of 8 suturing 3. Size > 6mm and > 48 hours: surgical closure : small defects – local flaps; large defects – regional/distant flaps Obturators: immunocompromised patients
- 45. In long-standing OAF we must evaluate the patient for maxillary sinusitis and treat it before closing the defect surgically The fistulous tract must be excised prior to surgical closure
- 46. • Most common and oldest surgical technique • Developed by Rehrman • Disadvantage: Reduces depth of buccal vestibule • Overall success rate approx. 87.2%
- 47. • Full thickness flap • Based on the greater palatine artery • Advantages: a) No reduction of vestibular depth b) Lesser chance of flap breakdown c) Anteriorly based flaps are ideal for closure of tuberosity defects • Disadvantage: Exposed palatal bone takes long time to heal
- 48. • First described by Egyedi in 1977 • Helpful in small to medium sized defects • Pedicled flap • Complication can be avoided: i. Graft should not be in tension ii. Patient should be on a liquid diet Anatomy of BFP: It has 4 processes- buccal, pterygoid, pterygopalatine, superficial and deep temporal Blood supply: Deep & superficial temporal artery, facial artery
- 49. • Based on lingual artery and its branches • Tongue flaps are useful : i. When both buccal and palatal flaps have failed ii. Defect size is > 1.5cm • Types of tongue flaps: a) Anteriorly based- Defects of hard palate, buccal mucosa b) Posteriorly based- Defects of soft palate • Disadvantages: i. Second surgery is required for flap division ii. Swallowing and speech difficulty • Some investigators placed the patients in IMF to reduced flap tearing
- 50. Gold foil
- 51. • By George Walter( USA, 1983) and Henri Luc (France,1989) • Technique to gain access to the maxillary antrum through canine fossa of maxilla • Indications: Removal of tooth fragments, chronic sinusitis, neoplasms, cysts Controlling maxillary antrum bleed/ haematomas Treating orbital floor fractures Nasal Antrostomy • Artificial ostium is made to the max. sinus with an opening in inferior meatus • Principle: Opening at a lower level improves drainage • Types : Middle meatal (child), inferior meatal, sublabial
- 52. Presented by: Dr Dibya Falgoon Sarkar
- 53. PNS Cysts Intrinsic cysts Mucocele Serous cysts Cholesteatoma Extrinsic cysts Dentigerous cysts Radicular cyst Neurogenic cysts Meningocele Encephalocele Fissural cysts Nasopalatine duct cyst Globulumaxillar cyst Median palatal cyst Pierse et al Oral & Maxillofacial Surgery Clinics 2012
- 54. Mucous retention cyst Mucous extravasation cyst (Mucocele) Most common and donot produce bone destruction Produces bone destruction Results from obstruction of glands in the sinus lining Results from accumulation of mucous in an obstructed sinus cavity Site: Floor of Maxillary sinus Site predilection: Frontal & Ethmoidal sinus Radiographically visible as a dome-shaped, homogenous mass Radiographically Pressure erosion seen surrounding sinus walls. Initially sinus is opacified • Treatment: Surgical excision along with the supplying gland • Excellent prognosis, low recurrence
- 55. Neurogenic cysts of PNS • Non-neoplastic lesions • Two types : Meningocele & encephalocele • Both are results of congenital herniation of intracranial meningeal and neural tissue • Encephalocele is more common and contains primitive neural tissue • Meningocele contains arachnoid and dural tissue and CSF • Radiographically seen as bony dehiscences in base of skull or cranial vault associated with a soft tissue extension in nose and PNS • Treatment : Surgical enucleation Encephalocele in fronto- ethmoidal sinus
- 57. Sinonasal tumours Benign tumours Epithelial tumors Sinonasal papilloma Mesenchymal tumors Osteoma Angiofibroma Haemangioma Malignant tumours Epithelial tumours Squamous cell carcinoma Adenoid cystic Carcinoma Adenocarcinoma Mesenchymal tumours Olfactory neuroblastoama Sarcomas
- 58. • Early : asymptomatic . • Oral symptoms: Toothache , trismus, alveolar ridge fullness, erosion , malocclusion . • Nasal findings: Obstruction, epistaxis, rhinorrhea , post nasal discharge , anosmia, nasal mass or polyposis, mass in the medical canthus, broadening of nasal dorsum . • Ocular findings: Epiphora, diplopia, proptosis • Facial signs: Paraesthesia, asymmetry • Maxillary sinus involvement: Mass in palate or upper alveolus . mass in upper gingivobuccal sulcus, malocclusion or loose teeth. • Advanced : Trismus, Orbital : Periorbital swelling , proptosis, epiphora , impaired ocular mobility
- 59. • Benign, localized proliferations of the respiratory mucosa • 10-25% of all paranasal tumors • Cause: Some clinicians believe that these are actually reactive hyperplasia secondary to stimulants like allergens, bacteria or HPV virus( type 6,11), tobacco smoking • Types : 1) Fungiform 2) Inverted 3) Cylindrical
- 60. Fungiform papilloma Inverted papilloma Cylindrical papilloma Distribution Similar to oral papillomas; 18-50% all PNS papillomas Most common, premalignant <7% of PNS papillomas HPV Almost all variants are HPV positve HPV 6,11,16 & 18 Low frequency of HPV association Age/sex 20-50 years; M>F > 20 years; M>F 20-50 years; M>F Clinical features Unilateral nasal obstruction, epistaxis, pink nodule Unilateral nasal obstruction, epistaxis, pink nodule, bone erosion, locally aggressive Unilateral nasal obstruction, epistaxis, robust red multi nodular Treatment Complete surgical excision, no malignant transformation Aggressive surgical excision, Greatest potential for malignant transformation and destruction Aggressive surgical excision
- 61. • Most common benign, mesenchymal tumor of PNS • Arises from junction of membranous & endochondral bone in frontoethmoidal suture region • May have intracranial/ orbital extensions • Histological subtypes: hard cortical & soft cancellous • Surgical excision • Low recurrence Osteoma Hard cortical osteoma Soft cancellous osteoma Lobulated densities obstructing sinus Less dense, may be mistaken with a soft tissue sinus mass
- 62. • Usually an extension of juvenile angiofibroma of nasopharynx • Often extends into sphenoid and ethmoidal sinuses • Have a vertical spreading pattern • Imaging: Appears as an enhancing lesion in MRI • Carotid angiography and CECT are helpful as angiofibromas contain a hypertrophied internal maxillary artery • Conservative surgical excision
- 63. • Rare mucosal neoplasm • Neural crest origin • Often exhibits immunological symbiosis with the host • Radical procedures are contraindicated • Treatment by endoscopic resection • Role of radiotherapy is debatable
- 64. • Arise from the nasal cavity (septum/ alveolus) • Multifocal, frequent recurrence • Spreads superiorly into skull base • Age range: both young and old • Treatment: Craniofacial resection • Not radiosensitive
- 65. • Classically arises from olfactory epithelium in the upper nasal vault • The presence of a mass in the upper nasal cavity with associated skull base erosion is typical. • Bimodal peak in the second/third and sixth/seventh decades. • Cervical metastases have been described in up to 23%. • These are routinely resected in craniofacial approaches • Endoscopic resection is being increasingly offered for this tumour particularly when it arises from the middle and superior turbinates. • Should always be combined with radiotherapy. Stage I confined to primary site Stage II presence of nodal metastasis Stage III presence of distant metastasis
- 66. • 3% of all the head and neck malignancies • Incidence: Maxillary sinus (70%), Ethmoid (20%), frontal (3%), Sphenoid(1%) • M > F ( 2 : 1 ) • Age – 6th & 7th decades • Risk factors : 1. Wood workers 2. Leather manufacturers 3. Smoking & alcohol • Damage from smoking and alcohol plays a less damaging role Case of Small cell neuroendocrine carcinoma of Left maxillary sinus
- 67. • About 30 per cent of patients with this condition are woodworkers. • These tumours usually arise in the middle meatus and spread into the ethmoidal sinuses • Adenocarcinoma is generally rather radio resistant but combined therapy is usually offered. • Many patients require a craniofacial but in selected cases have been treated successfully by an endoscopic resection • Use of topical 5- flurouracil and surgical debulking has been advocated
- 68. • Propensity to spread along perineural lymphatics which compromises attempts at excision. • Known to produce blood-borne metastases, classically to the lung while lymphatic spread is rare. • Treatment is generally combined surgery and radiotherapy
- 69. Clinical features: 1. Maxillary sinus ca • Accounts for 80% of all PNS cancers • Facial swelling, pain, paraesthesia of cheek • Epistaxis, nasal discharge, obstruction • Ill fitting dentures, alveolar/palatal mass • Proptosis, diplopia, impaired vision, orbital pain 2. Ethmoid sinus ca • Headache • Referred pain to nasal, retrobulbar region • Subcutaneous mass at inner canthus, diplopia & proptosis • Nasal obstruction, discharge,
- 70. 1. Tumors from maxillary sinus: • Posterior wall > Infratemporal fossa • Superior wall > Infraorbital canal > Orbit • Inferiorly > Roots of upper premolars & molars > Oral cavity / Palate 2. Tumors invading ethmoid bone: • Via lamina papyracea of ethmoid bone • Via emissary veins present anterior to the crista galli which eventually connects to the sagittal sinus • Via olfactory fibres through the cribriform plate 3. Tumors invading the orbit can spread via: • Superior orbital fissures > Cavernous sinus • Inferior orbital fissures > Pterygopalatine fossa & infratemporal fossa • Orbital apex > Middle cranial fossa 4. Tumors from nasal septum: • Superiorly: Into extranasal structures • Inferiorly: Into upper lip & gingivobuccal sulcus
- 71. Diagnostic work up for PNS carcinoma patients: • Routine blood examination • Histopathology • Chest X-ray for Adenoid cystic carcinoma • CT/MRI • Dental evaluation • Baseline ophthalmologic examination • Baseline speech & swallowing assessment • Fibre optic endoscopic examination & biopsy Lymphatic spread of PNS carcinoma: • Usually sparse-10% incidence of cervical lymph node metastasis • First echelon: Upper jugular/ submandibular nodes • Contralateral metastasis: extremely rare • Tumors of nasal septum, columella and nasal vestibule show bilateral metastases Lymphatic drainage of sinuses
- 73. AJCC stage Stage grouping Stage description 0 Tis N0 M0 The tumor is only in the top layer of cells lining the inside of the maxillary sinus and has not grown any deeper (Tis). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). I T1 N0 M0 The tumor has grown deeper, but it is only in the tissue lining the sinus (the mucosa) and does not grow into the bone. (T1). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). II T2 N0 M0 The tumor has begun to grow into some of the bones of the sinus, other than into the bone of the back part of the sinus (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0).
- 74. AJCC stage Stage grouping Stage description III T3 N0 M0 The tumor has grown into the bone at the back of the sinus (called the posterior wall) or into the ethmoid sinus, the tissues under the skin, or the side or bottom of the eye socket (T3). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). OR T1 to T3 N1 M0 The tumor might or might not have grown into structures just outside the maxillary sinus (T1 to T3). The cancer has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). IVA T4a N0 or N1 M0 The tumor is growing into the skin of the cheek, the front part of the eye socket, the bone at the top of the nose (cribriform plate), the sphenoid sinus, the frontal sinus, or certain parts of the face (the pterygoid plates or the infratemporal fossa). This is also known as moderately advanced local disease (T4a). The cancer has not spread to nearby lymph nodes (N0), or it has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0).
- 75. AJCC stage Stage grouping Stage description IVB T4b Any N M0 The tumor is growing into the throat behind the nasal cavity (the nasopharynx), the back of the eye socket, the brain, the tissue covering the brain (the dura), some parts of the base of the skull (middle cranial fossa or clivus), or certain cranial nerves. This is also known as very advanced local disease (T4b). The cancer might or might not have spread to nearby lymph nodes (any N). It has not spread to distant parts of the body (M0). OR Any T N3 M0 The tumor might or might not have grown into structures outside the maxillary sinus (any T). The cancer has spread to at least one lymph node that is larger than 6 cm across, OR it has spread to a lymph node and then grown outside of the lymph node (N3). It has not spread to distant parts of the body (M0). IVC Any T Any N M1 The tumor might or might not have grown into structures outside the maxillary sinus, and it might or might not have affected a vocal cord (any T). The cancer might or might not have spread to nearby lymph nodes (any N). The cancer has spread to distant parts of the body (M1)
- 77. • Nodal metastases is dependent upon histological subtype of the carcinoma Nodal metastases has as high as 28% in SCC, 25% in adenocarcinoma, 12% for undifferentiated carcinoma and 10% for adenoid cystic carcinoma. ( According to Kaplan et al AJCC 1999) • Maxilary sinus carcinomas involving hard palate shows a higher incidence of cervical node metastases (Castelnau et al Role of Elective Neck Management in Maxillary Sinus Squamous Cell Carcinoma. Otolaryngol (Sunnyvale). 2016) • Most powerful prognostic factor for overall survival is T- stage followed by nodal involvement (Wu TH, Huang JS, Wang HM, Wang CH et al Long-term survival after surgery of stage III-IV maxillary sinus carcinomaChang Gung Med J. 2010)
- 78. According to Jatin Shah et al 2015 (Curr Opin Otolaryngol Head Neck Surg 2015) • Treatment failure occurs in 62% of all cases of maxillary sinus carcinoma • Local recurrence is the most common cause • Thus they concluded that : 1. Elective treatment of neck is justifiable only in advanced staged (T3-4) maxillary sinus carcinomas 2. Elective neck dissection can be performed if we are planning for any vascular anastomosis in the neck during flap reconstruction 3. If neck is not entered in a case cN0 T3-4 tumor we should irradiate the neck during post op radiotherapy of primary site. IMRT is the most preferable modality of radiotherapy 4. Elective neck dissection is not recommended in T1-2 tumors of sinus
- 79. Incisions Midfacial degloving approach Weber –Fergusson approach Lateral rhinotomy approach Intra/extraoral Intraoral Extraoral Extraoral Access Indicated in pathologies of frontal, ethmoidal, maxillary sinus and infratemporal fossa Transoral approach for pathologies of maxilla, not suitable for skull base / ethmoid lesions Indicated for approach to maxillary, sphenoid and ethmoidal sinuses Advantages Excellent esthetics Easier and provides wide area of exposure Easier approach, scar lies in the folds of facial skin Disadvantages Technique sensitive Heals by scar formation, Limited access
- 82. Borle’s extension- When temporalis flap is planned for maxillectomy defect reconstruction Lynch extension- To expose the ethmoidal sinus Dieffenbach extension- When total maxillectomy is being planned
- 83. Palatal incisaion is given 3mm lateral to midline so that a mucoperiosteal flap is formed which can cover the raw bony edge Osteotomies through zygoma, floor of orbit, frontal process of maxilla & pyriform aperture
- 84. • The incision is made around the base of the nose (or entering the nostril floor for a better esthetical result) and along the facial nasal groove (In the border of both esthetic units). • The dissection goes deep to the subperiosteal plane of the frontal process of the maxilla. • Below the nasal bone the incision is deepened through the nasal mucosa. • A unilateral nasomaxillary osteotomy is made with a small osteotome, and the two osteotomy lines are joined at the level of the naso frontal junction. • The septum is cut and freed from the mobilized segment according to the resection plan
- 85. • Originally described by Tessier • Excellent approach for accessing the pathologies of frontal and ethmoidal sinuses. • Major risks of this approach include injury to the temporal and zygomatic branches of the facial nerve, temporal hollowing, scalp hematoma, parietal scalp pain, parasthesia or anesthesia, infection, and nasal orbital hypertrophy.
- 86. • First reported by Smith in 1954 • Has become a ‘gold standard’ for tumors affecting the anterior skull base ( According to Stell & Maran) • Principle: En bloc resection of the tumor including the ethmoidal sinuses, superior nasal septum and floor of anterior cranial fossa. • Laterally part of the bony orbit may also be included in anterolateral resection. • Indications: Malignant tumors requiring surgical resection and involving the anterior skull base • Contraindications: 1. Extensive frontal lobe involvement 2. Bilateral orbital invasion/ optic chiasm 3. Distant metastasis cases 4. Tumors with poor prognosis like malignant melanoma
- 87. • Incision: An extended lateral rhinotomy incision is made on the side of maximal tumor involvement.
- 88. • IMMEDIATE: – convulsions – haemorrhage – air embolism • INTERMEDIATE: – cerebrovascular accident – confusion – pulmonary embolism – meningitis • LONG TERM: – haemorrhage – frontal abscess/encephalitis – bone necrosis/fistula – cerebrospinal fluid leak – epilepsy – epiphora
- 89. Brown’s classification of Maxillectomy, 2010 (Lancet Oncol 2010; 11: 1001–08) Vertical classification: I—maxillectomy not causing an oronasal fistula; II—not involving the orbit; III—involving the orbital adnexae with orbital retention; IV—with orbital enucleation or exenteration; V—orbitomaxillary defect; VI— nasomaxillary defect. Horizontal classification: a—palatal defect only, not involving the dental alveolus; b—less than or equal to 1/2 unilateral; c—less than or equal to 1/2 bilateral or transverse anterior; d—greater than 1/2 maxillectomy. Letters refer to the increasing complexity of the dentoalveolar and palatal defect, and qualify the vertical dimension.
- 90. Algorithm for Maxillary Reconstruction (Brown JS, Richard Shaw; Lancet Oncol 2010; 11: 1001–08) • Class I defects: Most reconstructive techniques reported for class I defects are the fasciocutaneous radial forearm flap or obturators • Class II defects: 1) If the defect is less than half of the lateral alveolus and palate (class IIb), very good results can be achieved with either obturation or reconstruction. 2) Zygomatic implants are also efficient in Class II defects • Class III defects: a) With class III defects, orbital support is lost as well as anterior support of the cheek and dental arch. Very little role for a prosthetics. b) Vascularized bone grafts are ideal especially DCIA with internal oblique flap. • Class IV: Involve patients with stage IV disease and poor prognosis • Class V: Reconstruction with temporalis flap is adequate • Class VI: Nasomaxillary defects that involve the nasal bone with or without skin require reconstruction. Osteocut. RFFP is ideal.
- 91. Summary of published methods of reconstruction from 1998-2009, in number of reported cases Recommended methods by Brown et al.
- 92. Management algorithm of the PNS tumors invading the orbit (Stell & Maran)
- 93. • Can be used in resection of PNS tumours • May need combination with craniofacial resection if: 1. Dural invasion 2. Infiltration of superior sagittal sinus • Principles: Complete resection of the tumour including a wide field of clearance of adjacent mucosa, bone and cartilage • Can be used to repair skull base bone and dural defects • Extent of surgery: A complete fronto-ethmo- sphenoidectomy is undertaken with lateral nasal wall removal • Advantage: low morbidity and short hospital stay • Disadvantage: technique sensitive
- 94. • Extension through anterior cranial fossa • Involvement of both optic nerve • Posterior extension into sphenoid sinus • Invasion of middle cranial fossa • Inoperable neck node & distant metastasis • Well differentiated adenocarcinoma • Early maxillary tumors • Olfactory neuroblastoma • SCC arising from inverted papiloma
Editor's Notes
- Walls- a) Superior wall b) Anterolateralwall c) Posterolateralwall d) Inferior wall.
- Inferomedially- anterior lacrimal and post lacrimal crests
- Relations : i)Superiorly– optic chiasma & pituitary gland. ii)Inferiorly– roof of pharynx iii)On either side – cavernous sinus & internal carotid artery iv) Anteriorly – sphenoethmoidal recess v) Posteriorly – Pons & medulla
- Maxillary sinus- Light placed in sublabial region Frontal sinus- Light placed over supraorbital rim
- Affected sinus must be irrigated copiously with physiologic saline 3 times/day until inflammation subsides Antibiotics like Augmentin must be used Caldwell luc procedure must be done to removed infected sinus membrane prior surgical closure of OAC
- Cholesteatoma : Hyperkeratinised epithelium which completely replaces normal mucous membrane
- Neuroendocrine tumor, metabolites like VMA may be detected in urine Treatment: Craniofacial resection
- Radiotherapy delays recurrence
- 3 parts: intracartilaginous, transfixion incision, vestibular incision Limits of resecetion are posteriorly wall of sphenoid, pterygoid plates, superiorly skull base and laterally coronoid process of mandible Can be combined with coronal incision for craniofacial resection
- Extends 1cm lateral to lateral canthus & 3mm below lower eyelash Too close to lashes: ectropion; Too far: lower lid edema Orbicularis oculi is left intact but dissection is made at bony infraorbital rim Infraorbital neurovascular bundle is cut
- Described by Moure in 1902 Excellent access to nasal cavity through which a medial maxillectomy can be done Ant skull base, ethmoids, sphenoid & maxillary sinuses
- The soft tissues of the face are mobilized by subperiostial elevation to expose the nasal bones, frontal processes of the maxilla and frontal bone up to the hairline via an extended lateral rhinotomy. • Through the lateral rhinotomy, the upper lateral cartilage is separated from the nasal bone to allow complete retraction of the nasal ala. • The orbital periosteum is elevated to expose the lacrimal fossa and the medial orbital wall. The nasolacrimal duct is often transacted obliquely at this point • anterior and posterior ethmoidal arteries are divided after bipolar coagulation. • If the lamina has been eroded by tumour, the adjacent periorbita should be resected for frozen section assessment A shield-shaped craniotomy is performed above the level of the supraorbital rim to include the frontal sinus. usually approximately 3x3x3.5 cm size. • The frontal sinus which has been opened by this manoeuvre is cleared of its mucosa and the posterior wall removed combined with a wide dissection of the dura. The anterior and posterior ethmoidal arteries are coagulated with the bipolar diathermy although care must be exercised as the optic nerve is approached. Osteotomies are performed around the cribriform plate through the ethmoidal and sphenoid roofs. • The posterior osteotomy crosses the planum sphenoidale to include the anterior face of the sphenoid and the nasal septum is separated by quadrilateral cuts. • The specimen is mobilized this can be removed, haemostasis achieved and the cavity inspected for further resection. • fashion a large middle meatal antrostomy to prevent subsequent infection. • dura has small defects which can be repaired primarily but more with fascia lata held in place with fibrin glue to which a split-skin graft taken from the thigh is applied inferiorly.
- The most complex and controversial area in head and neck reconstructive surgery is the management of maxillary, midface, and skull-base tumours
- Should be regarded as major surgery equivalent to CRF resection via an endonasal route