z
Outline
Introduction
Embryology,Anatomy, Functions of the PNS
X – ray PNS
Indications
Occipitomental view
Occipitofrontal view
Lateral view
Submentovertex view
Special views
3.
z
Embryology
The maxillarysinus cavity is seen at birth on x-rays. They
increase in size till 14yrs of age.
The frontal is the last to get pneumatised and is visible only at
6years of age.
The sphenoid sinus is pneumatised by 2 yrs of age. Adult size
by 12-14 yrs.
The ethmoid sinuses are aerated by birth but are rarely visible.
They grow till 4 yrs of age and ha a growth spurt during
adolescence.
z
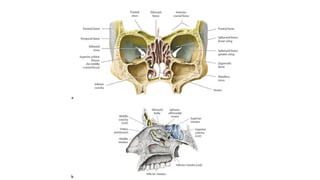
Anatomy of theparanasal sinuses
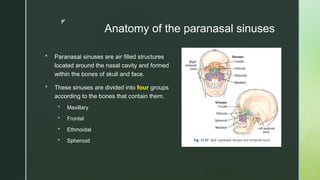
Paranasal sinuses are air filled structures
located around the nasal cavity and formed
within the bones of skull and face.
These sinuses are divided into four groups
according to the bones that contain them.
Maxillary
Frontal
Ethmoidal
Sphenoid
6.
z
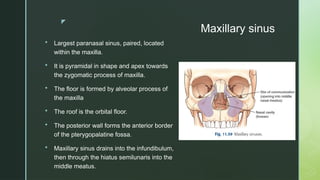
Maxillary sinus
Largestparanasal sinus, paired, located
within the maxilla.
It is pyramidal in shape and apex towards
the zygomatic process of maxilla.
The floor is formed by alveolar process of
the maxilla
The roof is the orbital floor.
The posterior wall forms the anterior border
of the pterygopalatine fossa.
Maxillary sinus drains into the infundibulum,
then through the hiatus semilunaris into the
middle meatus.
7.
z
Frontal sinus
Thefrontal sinuses are paired and are
present within the frontal bone.
Almost always asymmetrical and separated
by a septum.
Each sinus extends superior to the medial
end of the eyebrow and back into the orbital
region of the frontal bone.
Frontal sinus drains through the nasofrontal
duct, which can, in turn, drain into either the
frontal recess or ethmoid infundibulum and
then into the middle meatus.
8.
z
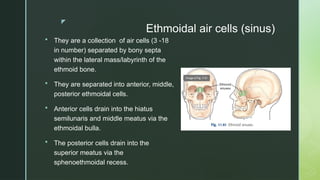
Ethmoidal air cells(sinus)
They are a collection of air cells (3 -18
in number) separated by bony septa
within the lateral mass/labyrinth of the
ethmoid bone.
They are separated into anterior, middle,
posterior ethmoidal cells.
Anterior cells drain into the hiatus
semilunaris and middle meatus via the
ethmoidal bulla.
The posterior cells drain into the
superior meatus via the
sphenoethmoidal recess.
9.
z
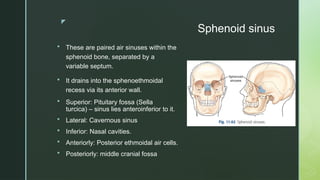
Sphenoid sinus
Theseare paired air sinuses within the
sphenoid bone, separated by a
variable septum.
It drains into the sphenoethmoidal
recess via its anterior wall.
Superior: Pituitary fossa (Sella
turcica) – sinus lies anteroinferior to it.
Lateral: Cavernous sinus
Inferior: Nasal cavities.
Anteriorly: Posterior ethmoidal air cells.
Posteriorly: middle cranial fossa
11.
z
Functions of theParanasal sinuses
Air conditioning of the inspired air by providing a large
surface area over which the air is humidified and warmed.
Resonance to voice.
Act as thermal insulators to protect delicate structures within
the orbit and cranium for variations in the intranasal
temperature.
Lightens skull bones.
12.
z
X – RayPNS
Currently the utility of radiographs is limited.
The sensitivity and specificity of plain radiographs is low.
In a properly exposed radiograph, PNS density is identical to
orbital density.
Abnormalities manifest as opacification of sinuses, bone
destruction,soft tissue or displacement of structures.
13.
z
X – RayPNS
Standard four views of the x – ray pns include:
Occipitomental view (Water’s view)
Occipitofrontal view (Caldwell’s view)
Lateral view
Submentovertical view
14.
z
Indications
Sinusitis –To detect mucosal thickening, fluid levels or
opacification
Sinus/polyps – soft tissue mass within sinus visible
Trauma
Foreign body
15.
z
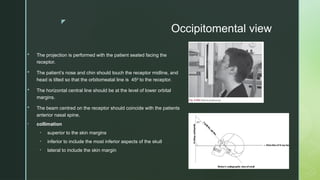
The projectionis performed with the patient seated facing the
receptor.
The patient’s nose and chin should touch the receptor midline, and
head is tilted so that the orbitomeatal line is 45 to the receptor.
⁰
The horizontal central line should be at the level of lower orbital
margins.
The beam centred on the receptor should coincide with the patients
anterior nasal spine.
• collimation
• superior to the skin margins
• inferior to include the most inferior aspects of the skull
• lateral to include the skin margin
Occipitomental view
18.
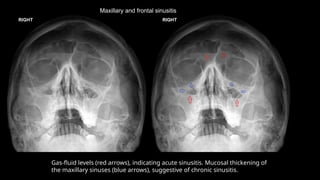
Maxillary and frontalsinusitis
Gas-fluid levels (red arrows), indicating acute sinusitis. Mucosal thickening of
the maxillary sinuses (blue arrows), suggestive of chronic sinusitis.
19.
z
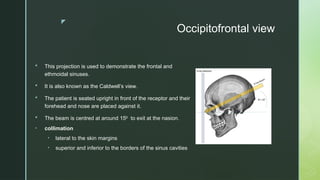
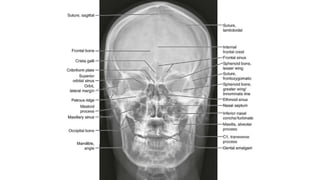
Occipitofrontal view
Thisprojection is used to demonstrate the frontal and
ethmoidal sinuses.
It is also known as the Caldwell’s view.
The patient is seated upright in front of the receptor and their
forehead and nose are placed against it.
The beam is centred at around 15 to exit at the nasion.
⁰
• collimation
• lateral to the skin margins
• superior and inferior to the borders of the sinus cavities
22.
Two frontal viewsof the skull demonstrate an incidental rounded, sclerotic lesion growing into the right frontal sinus (white arrows).
23.
z
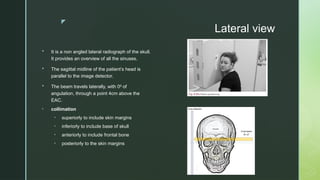
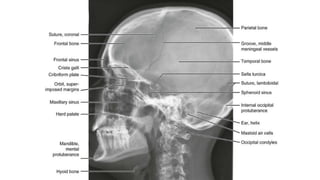
Lateral view
Itis a non angled lateral radiograph of the skull.
It provides an overview of all the sinuses.
The sagittal midline of the patient’s head is
parallel to the image detector.
The beam travels laterally, with 0 of
⁰
angulation, through a point 4cm above the
EAC.
• collimation
• superiorly to include skin margins
• inferiorly to include base of skull
• anteriorly to include frontal bone
• posteriorly to the skin margins
26.
Air fluid levelsseen on lateral view indicating skull base fracture
27.
z
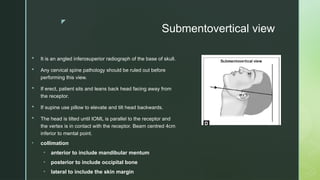
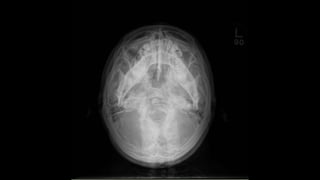
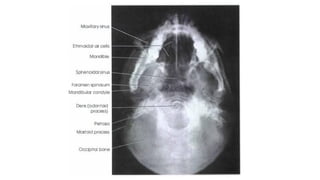
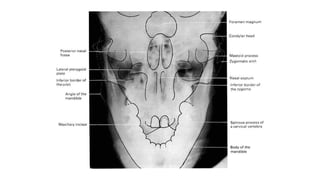
Submentovertical view
Itis an angled inferosuperior radiograph of the base of skull.
Any cervical spine pathology should be ruled out before
performing this view.
If erect, patient sits and leans back head facing away from
the receptor.
If supine use pillow to elevate and tilt head backwards.
The head is tilted until IOML is parallel to the receptor and
the vertex is in contact with the receptor. Beam centred 4cm
inferior to mental point.
• collimation
• anterior to include mandibular mentum
• posterior to include occipital bone
• lateral to include the skin margin
z
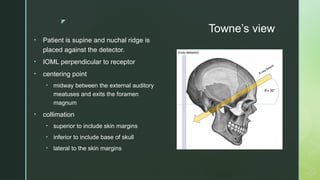
Towne’s view
• Patientis supine and nuchal ridge is
placed against the detector.
• IOML perpendicular to receptor
• centering point
• midway between the external auditory
meatuses and exits the foramen
magnum
• collimation
• superior to include skin margins
• inferior to include base of skull
• lateral to the skin margins
35.
z
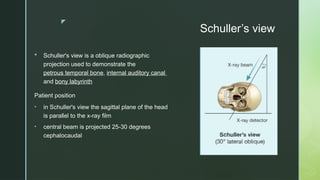
Schuller’s view
Schuller'sview is a oblique radiographic
projection used to demonstrate the
petrous temporal bone, internal auditory canal
and bony labyrinth
Patient position
• in Schuller's view the sagittal plane of the head
is parallel to the x-ray film
• central beam is projected 25-30 degrees
cephalocaudal

































![Radiography of skull [Autosaved].pptxriuyowioehgg](https://cdn.slidesharecdn.com/ss_thumbnails/radiographyofskullautosaved-251211014507-1d75cfe3-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









