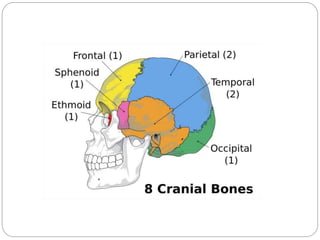
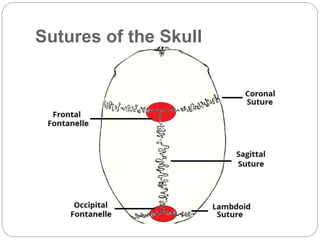
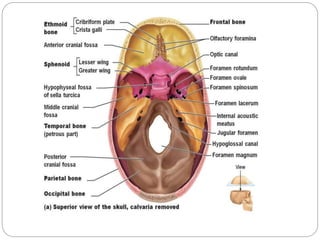
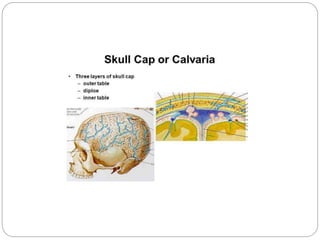
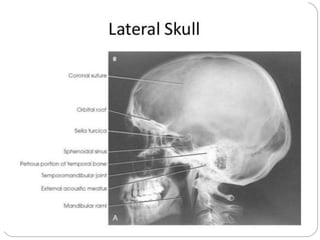
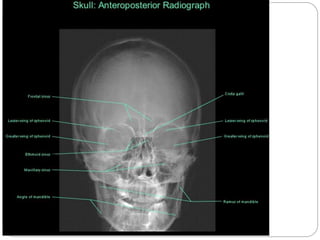
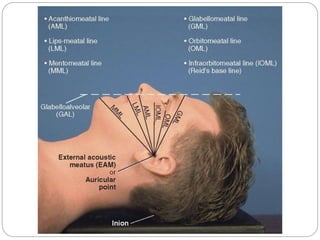
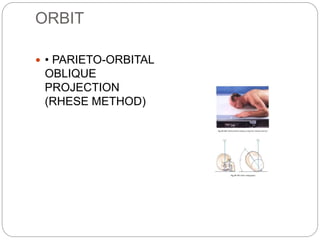
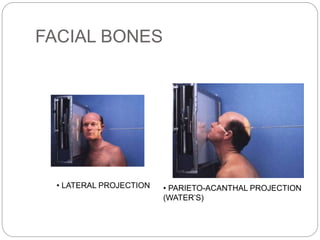
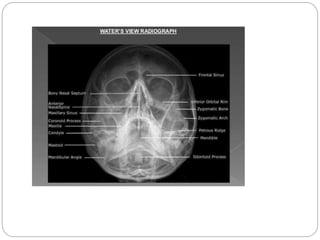
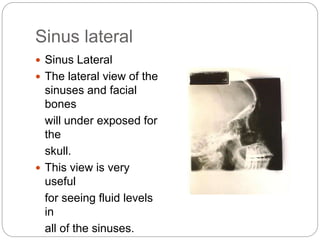
This document provides an overview of skull anatomy and various radiological projections used to image the skull. It describes the 22 bones that make up the skull, including landmarks like the nasion, glabella, and external occipital protuberance. Common projections are discussed like the PA, lateral, Towne, and Caldwell views. Specific positioning considerations and structures visualized are outlined for each view. Other projections for detailed examination of regions like the orbits, sinuses, facial bones and temporomandibular joints are also mentioned.
















































































![Radiography of skull [Autosaved].pptxriuyowioehgg](https://cdn.slidesharecdn.com/ss_thumbnails/radiographyofskullautosaved-251211014507-1d75cfe3-thumbnail.jpg?width=640&height=640&fit=bounds)





















