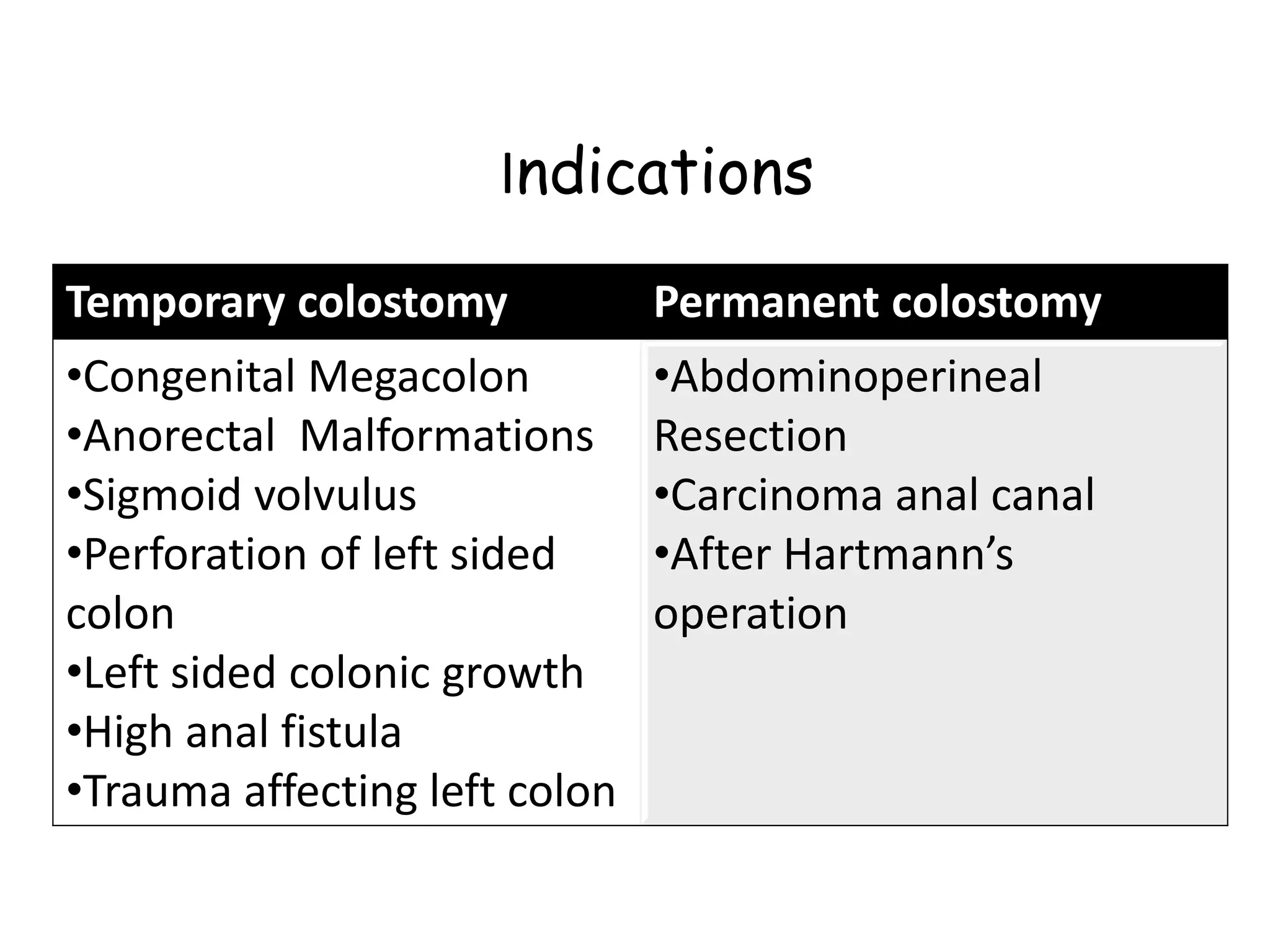
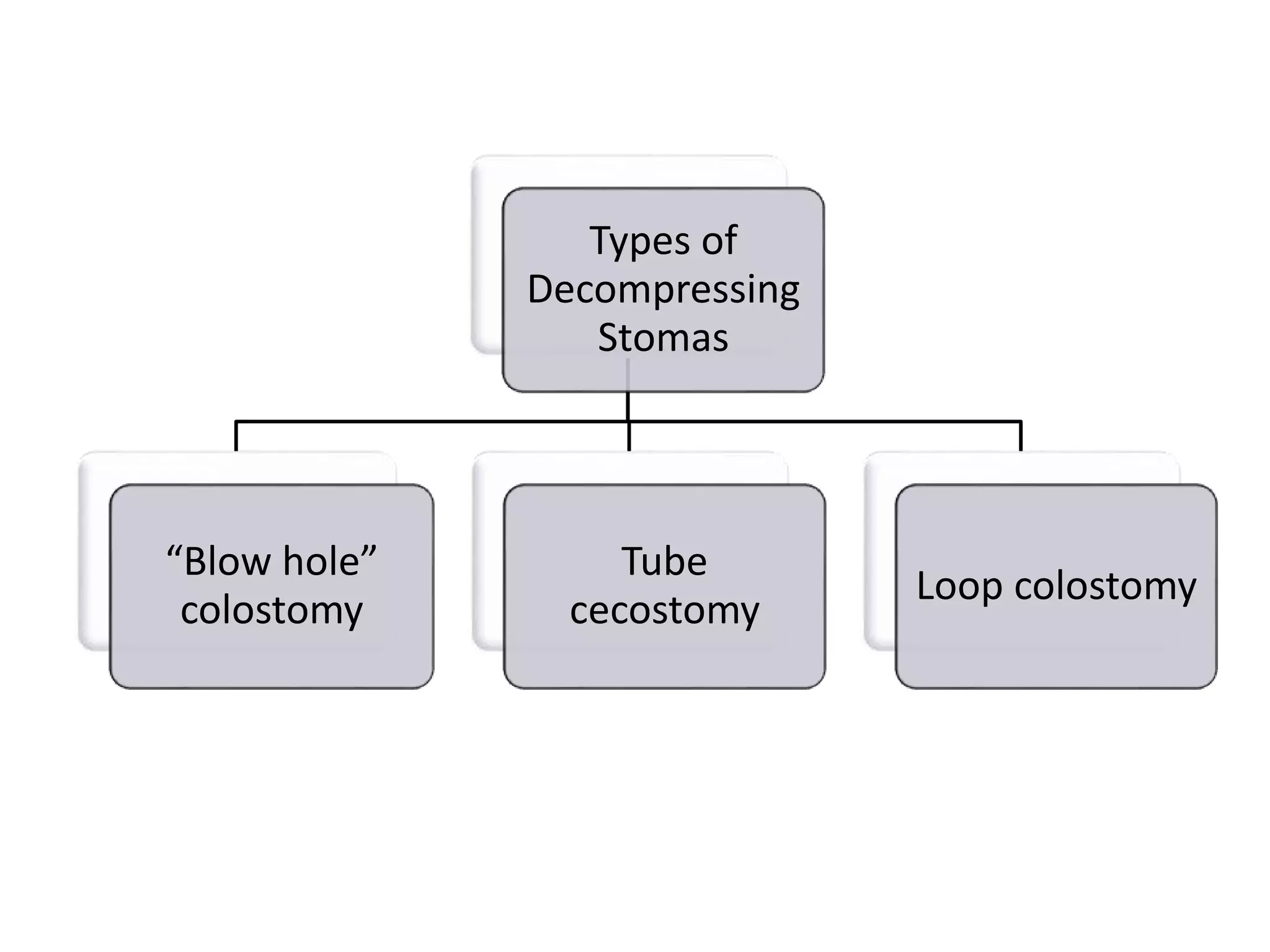
This document discusses colostomies, which involve connecting the colon to the abdominal wall for drainage of fecal matter. It describes why colostomies are constructed on the abdominal wall rather than in the perineum, the various types of colostomies based on location and function, and how different types like end colostomies, loop colostomies, and blowhole cecostomies are constructed. Temporary colostomies are usually closed after 3 months once the underlying condition is resolved and the distal colon has healed.























































![Basics of Stoma and Management care[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/basicsofstomaandmanagement1-250417022629-8799f789-thumbnail.jpg?width=640&height=640&fit=bounds)


























