This document discusses water and electrolyte balance in the human body. It covers the following key points:
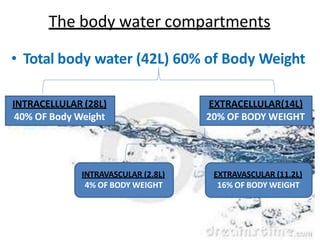
- The body is composed of 60-70% water distributed between intracellular and extracellular fluid compartments.
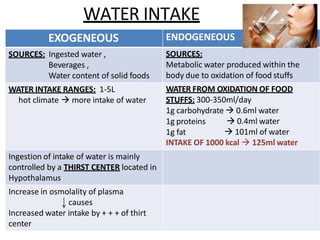
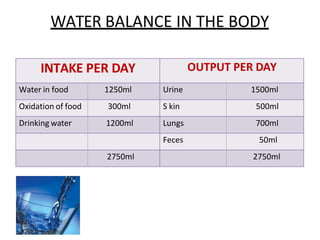
- Water intake and output is carefully regulated to maintain balance, with intake from food/beverages and output primarily through urine, skin, lungs and feces.
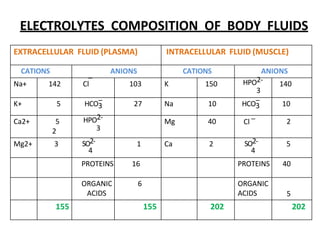
- Electrolytes such as sodium, potassium and chloride are important components of body fluids and their levels are maintained within a narrow range.
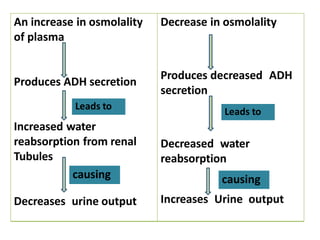
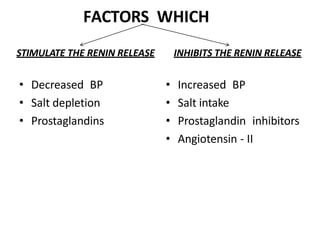
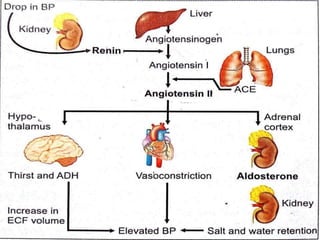
- Hormones like aldosterone, ADH and the renin-angiotensin system help regulate sodium and water balance.
- Abnormalities in electrolyte levels can
![CLINICAL SIGNIFICANCE
• ACE (Angiotensin Converting Enzyme) is a
glycoprotein.
• ACE inhibitors is useful in treating EDEMA &
CHRONIC CONGESTIVE CARDIAC FAILURE.
• Peptide Analog of Angiotensin-II [SARALASIN] &
antagonists of the converting enzyme [CATOPRIL]
are useful in treating Renin-Dependent
hypertension.](https://image.slidesharecdn.com/waterandelectrolytebalance-230320045425-734aedb7/85/waterandelectrolyte-balance-pptx-24-320.jpg)