Downloaded 169 times






































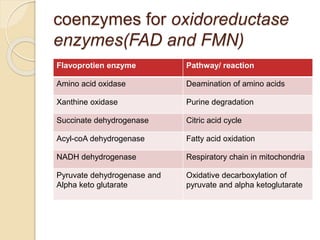
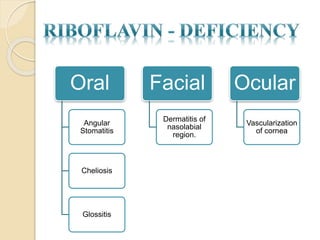







This document provides information on B-complex vitamins, including their classification and properties. It then focuses on thiamine (B1) and riboflavin (B2), discussing their history, structures, roles as coenzymes, dietary sources, deficiencies, investigations and treatments. For thiamine and riboflavin, key details are provided on their specific coenzymes, metabolic reactions they participate in, risk factors for deficiency, clinical signs, recommended intake levels, and management approaches. The document synthesizes information from various biochemistry textbooks and references.
































![VITAMINB2[RIBOFLAVIN] MEDICINAL CHEMISTRY,BY P.RAVISANKAR [SOURCES OF VITAMI...](https://cdn.slidesharecdn.com/ss_thumbnails/vitaminb2-pptravisankarvignanpharmacycollge-130615122609-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)