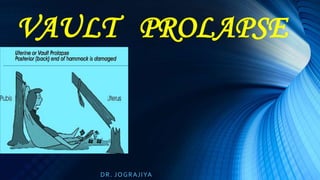
Vault prolapse, Pelvic organ Prolapse, Supports Of Uterus
•Download as PPSX, PDF•
74 likes•15,516 views

Vault Prolapse, Pelvic organ Prolapse, Supports Of Uterus

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Vault prolapse, Pelvic organ Prolapse, Supports Of Uterus
Similar to Vault prolapse, Pelvic organ Prolapse, Supports Of Uterus (20)
Recently uploaded
Recently uploaded (20)
Vault prolapse, Pelvic organ Prolapse, Supports Of Uterus
- 2. INTRODUCTION • It is most distressing to find a patient coming back with complaints of SCOPV after a hysterectomy • The first reaction of the doctor is to disbelieve the symptom and give it a short shrift • Tackling of vault prolapse (VP) is relatively rare and uncommon • Knowing the aftermaths of hysterectomy it takes time for a Gynecologist to mentally get tuned to the fact that patient requires repeat surgery
- 3. • The dilemma faced is whether to go abdominally or vaginally (million dollar question.) • Pelvic floor disorders continue to become even more prevalent as women lead longer lives. • Lifetime risk of surgery for pelvic organ prolapse is 11%. • Re-operation rate for failure is 29%. • Thorough understanding of the pelvic anatomy and relationship of vagina is imperative.
- 4. Evolution • From quadriped to biped with loss of tail------ • Loss of muscle in iliococcygeus, pyriformis and coccygeus. • Change in type of muscles of levator ani • Change in configuration of endopelvic fascia.
- 5. Relevant Anatomy • Pelvis is divided into false and true pelvis. • In upright position angle between inlet and outlet is 15-20 degrees. • Bony landmarks of importance — - Ischial spines and tuberosity - Sacral promontary - S1-S2
- 6. • Pelvic Ligaments – condensation of visceral connective tissue that assume special supportive role. - Sacrospinous lig. - Sacrococcygeus lig. - ArcusTendinous Fascia Pelvis - ArcusTendinous Levator Ani - Cardinal / Utero-sacral ligament
- 7. • Levator Ani Muscle –forms pelvic floor - predominantly type 1 muscle fibres - are in a state of constant Contraction. - flap-valve effect- by normal tone of ms and adequate depth of vagina. • During periods of increased abdominal pressure,upper vagina is compressed against levator plate. “The Posterior Pelvic Floor is the Achilles heel of the Pelvic diaphragm because of its vulnerability during Child Birth & Aging . ….Max Bloom
- 8. Urogenital diaphragm - Is a dense fibromuscular tissue that spans the opening of the anterior pelvic outlet - it consists of – Perineal body and 2 strap muscles – compressor urethrae, sphincter urethrae
- 9. PELVIC CONNECTIVE TISSUE Visceral fascia – collagen,elastin,adipose tissue, smooth ms Helps in expansion of organs Reduced smooth ms predisposes to Laxity and prolapse Parietal fascia – organized arrangement Of collagen, proteoglycans increase in type 3 collagen predisposes To laxity and prolapse
- 10. • Fascia – - Pubovescico-cervical - Paravaginal fascia - Rectovaginal fascia - Recto-vaginal septum
- 11. De Lancey vaginal supports. Level Support Defect 1 Proximal(upper) Paracolpium ligs USL & Cardinal. .UV prolapse .vault prolapse .enterocole 2 Mid-Vaginal Lat attachment to pelvic side wall to ATFP, ATLA Anterior & post wall defects & SUI. 3 DistalVaginal Pubocx fascia & RVS fusion to UGD , PB Lax perineum, low rectocoele, anal incontinence.
- 12. “Pelvic Organ Prolapse is often a reflection of our Obstetrical Incompetence” ……Lean Van Dongen ETIOLOGY: • Increasing parity - 1.2 times risk with each vaginal delivery. - 8.4 times with 2 vaginal deliveries (Oxford Family Planning – Mant 1997) - 11.4 times with 4 vaginal deliveries (Turkish study – Erata 2002)
- 14. •In vaginal delivery pelvic floor exposed to compressive and expulsive forces. 238 – 403 mmHg. •Prolonged 2nd stage- O2 deprivation causes necrotic changes. Ms , paravaginal tissue severely atrophied or dysfunctional. •Pudendal neuropathy following delivery.
- 16. • Macrosomia • Epidural analgesia • Instrumental deliveries & Oxytocin, PG augmentation • Age- risk increases 8% at 40yrs,11% at 50yrs. Due to hypoestrogenism, degenerative and organic diseases related to aging. • Genetic predisposition- weak fascia,collagen (type 3) or muscle(type 1). “Good obstetrician is the essence of preventive gynaecology” (Novak)
- 17. • Chronic increased intra abdominal pressure- obesity, constipation, COPD,Hypothyroidsism, lifting heavy weight. • Following hysterectomy , secondary hypotrophy of the cardinal- uterosacral ligament complex .(iatrogenic)
- 18. •Separation of pubocervical fascia from rectovaginal fascia causes apical enterocoele, commonly seen in post- hysterectomy patients, hence, essential to get them together with the vaginal muscularis and the uterosacral ligs.
- 20. PRESENTING SYMPTOMS • Apical VP • More anterior vaginal wall prolapse • Enterocele with posterior vaginal wall prolapse • All of above with lax perineum • All of above with laxity of introitus (puborectalis or bulbocavernous)
- 21. Evaluation • Pre-operative assessment of sites of damage by POPQ.
- 22. POPQ
- 24. Stages of POP–Q system measurement Stage 0 no prolapse is demonstrated Stage 1 the most distal portion of the prolapse is > 1 cm above the level of the hymen Stage 2 the most distal portion of the prolapse is 1 cm or less proximal or distal to the hymenal plane(> -1 but <1 cm) Stage 3 the most distal portion of the prolapse protrudes more than 1 cm below the hymen but protrudes no farther than 2 cm less than the total vaginal length [>+1 but <+(tvl-2cm)] Stage 4 vaginal eversion is essentially complete [≥+(tvl-2)]
- 25. Site Specific Prolapse Repair CYSTO/RECTOCOELE - Dislocation - Overdistention CAUSE • Damage to lateral Destruction of fibromuscular elasticity support with increase total length & width of vag wall & fornices connective tissue CORRECTION • Restoration of vaginal Reduction of width depth, axis and support. Inverted ‘T’ Repair Parachute Repair
- 26. Cont. Evaluation • Determine pre-operatively whether lower urinary tract dysfunction and defecatory dysfunction co-exist. • Configuration of – abdominal wall, sacral promontary, ischial spine, depth of pelvis and previous surgery with resultant adhesions. • Dynamic analysis by MRI. Technical error- patient is evaluated in recumbent rather than standing position. Dynamic pelvic floor fluoroscopy . Also accurately identifies enterocoele.– Done abroad.
- 27. ENTEROCOELE WITH VP Type Location Treatment Congenital Btwn post vag wall & ant rectal wall Excision of sac with high ligation & approximation of USL Pulsion Eversion of vault Culdoplasty if ligs strong If poor support then do sacrospinous fixation Traction Cysto & recto pulling vault into eversion In addition anterior and posterior colporrhaphy. Iatrogenic Change in axis of vag Obliterate sac & restore axis.
- 28. Classification of Vault Prolapse • 1st degree – vaginal apex is visible when perineum is depressed. • 2nd degree – apex extends just through the introitus. • 3rd degree – upper 2/3rds of the vagina is outside the introitus. • 4th degree – entire vagina is outside the introitus
- 29. Prediction with reasonable accuracy in VH – who will develop Vault Prolapse - Bonney • Pt. in lithotomy posn. • Reposit procidentia in pelvis • Ask pt. to bear down or cough. • Observe what protrudes out first. • If cervix, uterus or vault appear first- level 1 damage ( card / USL)- Primary Pexy with surgery • If cystocele , rectocele appear first- level 2/3 damage ( pelvic diaphragm)-VH with AP repair adequate
- 30. Choice and Route of Surgery • No general consensus on best procedure • Choice of surgery depends on- - Comfort & skill of surgeon - Primary or recurrent prolapse - Patient factor : age, health status , state of tissues, sexual activity. • Transvaginal route safer- VP aft. Vag hyst • Transabdominal route for – VP after abdo. hyst., lap hyst., harmonic vessel seal - Failure of previous vaginal approach - Foreshortened vagina. “Surgery is Anatomy Practically Applied” …Campbell
- 31. DIFFICULTIES DURING SURGERY • VAGINAL APPROACH • Post menopausal atrophic vagina • Skimpy Pubovesical fascia and absence of support to bladder base (as uterus absent)-difficult to take buttressing sutures during A repair. • Incomplete receding of bladder bulge even after repair (Surgeon does not have satisfaction of doing a complete repair). “ABILITY AND NECESSITY DWELL NEAR EACH OTHER “ ….Pythagoras
- 32. VAGINAL APPROACH DIFFICULTIES….. •‘Hypoestrogenic vagina , attenuated uterosacral ligaments-enterocele sac separation difficult • Occasional impaction of intestine with adhesion in POD , - difficult and dangerous to approach sac - difficult in enterocoele repair - often incomplete •Thinned out Dennonvillers fascia makes buttressing sutures of rectocele repair untenable.
- 33. VAGINAL APPROACH DIFFICULTIES… • Sacrospinopexy - Obesity, ATROPHIC vagina, para vagina loose areolar tissue and coccygeal sacrospinal complex– increase chances of failure. - osteoporosis (old age) of ischial spines- periosteitis. - malpositioning of pudendal /gluteal vessels and nerves. - Anatomy relatively unexplored
- 34. ABDOMINAL APPROACH DIFFICULTIES • Old age High risk for anesthesia & surgery • Obesity, pendulous abdomen • Loss of abdominal muscle tone • Venous stasis & vascular impedence – increased Oozing in Retroperitoneal space • Osteoporosis – periosteitis at site of sacropexy
- 35. ABDOMINAL APPROACH DIFFICULTIES… • Bladder and rectum adherent to vagina and overhang the vault– difficulty in locating the vaginal vault and dissecting the anterior and posterior vaginal walls. • Ureters –medial ,close to apex with fibrosis of adjacent fascia- chances of ureteric damage when passing sling needle. • Uterosacral ligaments attenuated & shortened. • Posterior peritoneum puckered , needle difficult to pass. • Round ligament shortened and bladder overhanging– pexy difficult
- 36. PREVENTION • Preoperative Bonneys Assessment • Paracolpium (endo.Fascia +vag. Mus supports vault following hysterectomy provided it is effectively attached to the vault. • Thorough reassessment of sites of damage prior to hysterectomy achieves a more perfect RECONSTRUCTION. • Keep Adequate vaginal length. “The operative treatment of prolapse has been the mirror of our knowledge of pelvic anatomy”….George Noble
- 37. • Adequate Repair of cystocoele/rectocoele and vault hook up. • Anterior vagina sits and derives support from an adequate posterior wall. Anterior colporrhaphy should be followed by repair of demonstrable damage to posterior wall. Failure to do so- reoperation in later years. • Take care during non descent hysterectomy • When vessel seal/ harmonic opted for do not forget buttressing vault. • In Lap. hyst, suture uterosacrals to vaginal vault. P R E V E N T I O N
- 39. VAGINAL •McCall’s culdoplasty •Sacrospinous ligament fixation •High Uterosacral ligament suspe- - nsion with fascial reconstruction •Iliococcygeus fascia suspension •Meshplasty
- 40. ABDOMINAL • Abdominal sacral colpopexy • High uterosacral ligament suspension • Laproscopic approach
- 41. OBLITERATIVE •LeFort’s Partial Colpocleisis •Introital tightening •Colpectomy
- 42. P1000701.jpg McCall Culdoplasty • A wedge of posterior vaginal wall and peritoneum removed • Enterocole sac freed and excised • Two internal sutures (permanent) placed approximating both USL and posterior peritoneum. • One external suture thru USL , post peritoneum & brought out thru post vaginal wall. • This obliterates cul-de-sac, supports vaginal apex P1000701.jpgP1000701.jpg
- 43. High USL fixation with fascial reconstruction (Richardson) • Identifying defect in endopelvic fascia • Reducing enterocoele sac • Closing fascial defect • Resuspension of vagina to original level 1 support • Non absorbable sutures put through USL at level of ischial spine and tied across in midline to form a ridge to which vagina is to be anchored • Absorbable sutures are used to suspend ant. And post. Vaginal walls to the USL ridge. • These are tied to suspend vagina in the hollow of sacrum • Perform cystoureteroscopy to evaluate ureteral integrity.
- 44. Sacrospinous ligament fixation • Principles to follow while dissecting to reach sacrospinous lig- work lateral to rectal wall - go posterior to uterosacral ligs - start dissecting cranial to levator belly, pierce pararectal ligament. Locate SSL. • Taking sutures thru SSL • Suspending the vault with pulley stitch or placing sutures thru full thickness of vagina. • Other Pexy : vagina to pelvic fasc: Shull, • Vagina to sacrotuberous : Amreich • Vagina to arcus tendinous : White • Vagina to sacrospinous lig: Richter
- 45. Iliococcygeus fascia suspension (Inmon) • Repair any anterior compartment defect • Iliococcygeus ms identified lateral to rectum & anterior to ischial spine • Sutures placed anterior to ischial spine • Passed thru vaginal apex
- 46. Meshplasty • MRI and CT delineation of defects in the fascial planes causing anterior or posterior defects – precise positions of defects which are difficult to correct, • Hence, proponents feel meshes are ideal • Apogee: for posterior defect • Perigee : for anterior defect • PROLIFT and likes: for vault prolapse • Is beset with its own problems and complications
- 47. • Apex of vault held with Allis and pushed up. • Incision-Infraumbilical midline incision taken • Preparation of vaginal vault – - Peritoneum over vault incised - Plane developed between posterior wall & rectum - Bladder base dissected off the superior aspect of anterior vagina • Preparation of sacrum – - sigmoid pushed to left - peritoneum over promontary & 1st 3 sacral vertebrae incised & continued to vaginal incision. Abdominal Sacral Colpopexy
- 48. • Placement of mersilene tape / mesh – - length 3X15cms. - tape/ mesh sutured to vaginal tissues using full thickness interrupted non-absorbable sutures. - continue anteriorly taking care of any cystocoele - tape/ mesh turned back towards apex & then towards the sacrum - secured to sacrum • Reperitonealisation done.
- 49. High USL fixation with fascial reconstruction Reducing enterocoele sac by multiple sutures through USL Closing fascial defect Resuspension of vagina to original level 1 support
- 50. Laparoscopic approach • Rise in adoption of laparoscopic approach. • Advantages- Improved haemostasis • improved visualization of anatomy • Reduced hospital stay, post-operative pain • Reduced overall cost • Disadvantages- technical difficulty in retroperitoneal dissection • steep learning curve • Increased operative room time increasing cost. • Risk of injury to vital structures.
- 51. LeFort Colpocleisis / Colpectomy • Small Kelly’s Repair—SUI • Marking out rectangular / triangular flaps on Anterior and posterior vaginal walls • Repeated sucessive stitches to invert the tissues • Suturing of uppermost horizontal part of rectangular flaps to each other with delayed absorbable sutures. • Small P repair, if necessary • To supplement , do introital tightening if extreme laxity
- 52. COMPARATIVE STUDY of 56 CASES (23-A, 33-V) AP REPAIR enterocele correction and USL pli in SACROSPINO PEXY with/ out AP Repair ABDOMINAL SACROCOLPO PEXY with/out AP Repair Kelly’s + COLPO CLEISIS with introital tightening INDICATION Ant. & post. Defect , apex pulled up Following VH , good vag length Following abdo/ lap. Hyst. Aged pt. high risk NUMBER OF PTS 17 12 15 12 DIFFICULTY IN SURGERY 0 4 8 0 SUBJECTIVE RESPONSE Fair Good Good Good COMPLICATIONS to look out for bleeding Incompl repair Hunt for atten USL Pudendal vs injury Sciatic nerve injury Bleeding Anatomical distortion Adhesions Difficult fixation (sacral and vaginal) Minimal bleeding Prevent over correction FAILURE SUBJECTIVE 12.2% 9.6% 8.3% 9.1% FAILURE ABSOLUTE: RECURRENCE OFV.P. ….. 3 (5.35%)
- 53. Pointers to successful surgery • Age • Proper counselling • High risk factors • Previous surgeries performed • No. of attempts at repair • Symptoms and signs • Type of vault prolapse • Defects in supports identified • Skill, knowledge and experience of surgeon • Comfort, confidence with particular surgery
- 54. •THE BEST DEFENCE IS A GOOD SURGICAL OFFENSE •No stereotyping patients, - INDIVIDUALISATION - the NEED ! •SURGERY SHOULD FIT THE PATIENT , THE PATIENT SHOULD NOT FIT THE SURGERY. - Michael Smith