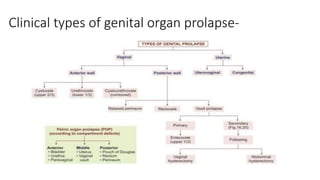
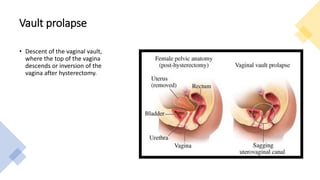
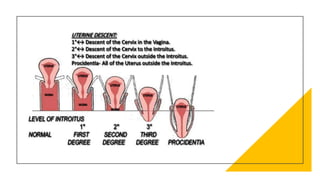
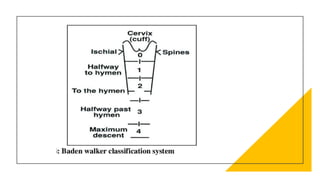
This document discusses displacement of the uterus. It begins by defining version and flexion of the uterus. It then discusses genital prolapse, describing the three levels of support for the uterus. It outlines the clinical types of genital organ prolapse including anterior and posterior vaginal wall prolapse as well as vault prolapse. It discusses the etiology, symptoms, diagnostic approach, and treatment options which include pessary, physiotherapy, and various surgical procedures. Ayurvedic view on pathogenesis and treatment involving local application of ghrita, swedana, and bandaging is also summarized.