Downloaded 130 times

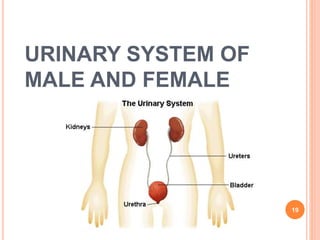
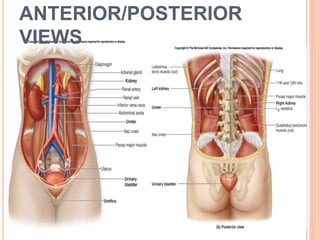
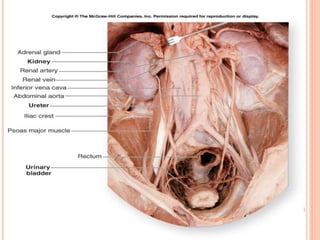
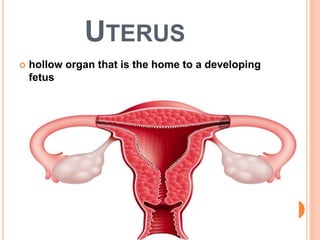
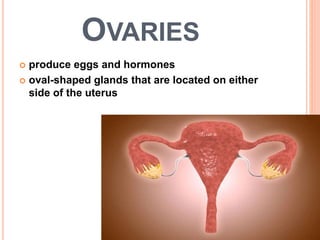
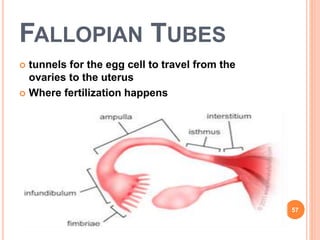



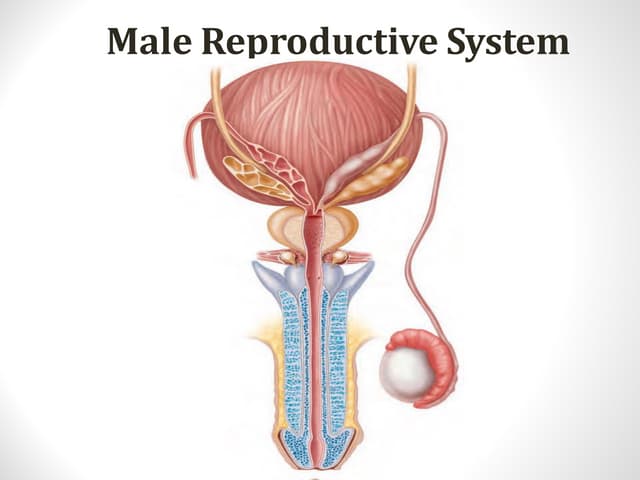
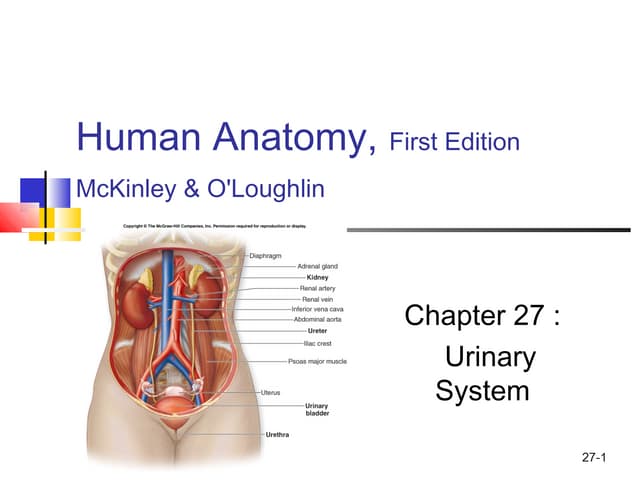
This document provides an overview of the male and female urogenital systems. It describes the anatomy and functions of the kidneys, bladder, urethra, prostate, testes, ovaries, and other reproductive organs. It also discusses clinical examinations, common pathologies like urinary tract infections and prostate issues, and diagnostic tests. The male and female reproductive processes are outlined, from sperm and egg production through fertilization. Overall, the document serves as an introductory guide to the anatomy and clinical aspects of the urogenital system.