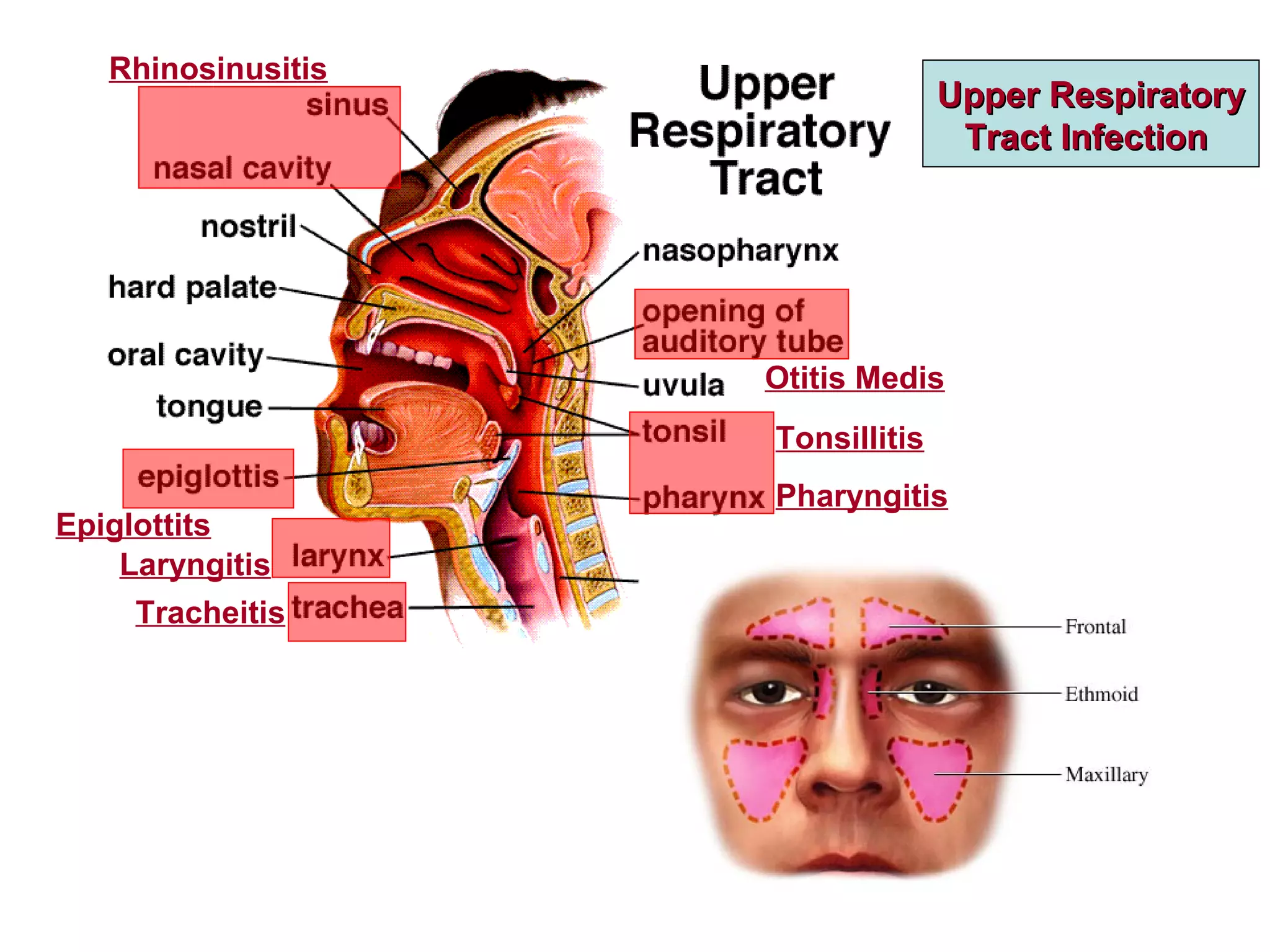
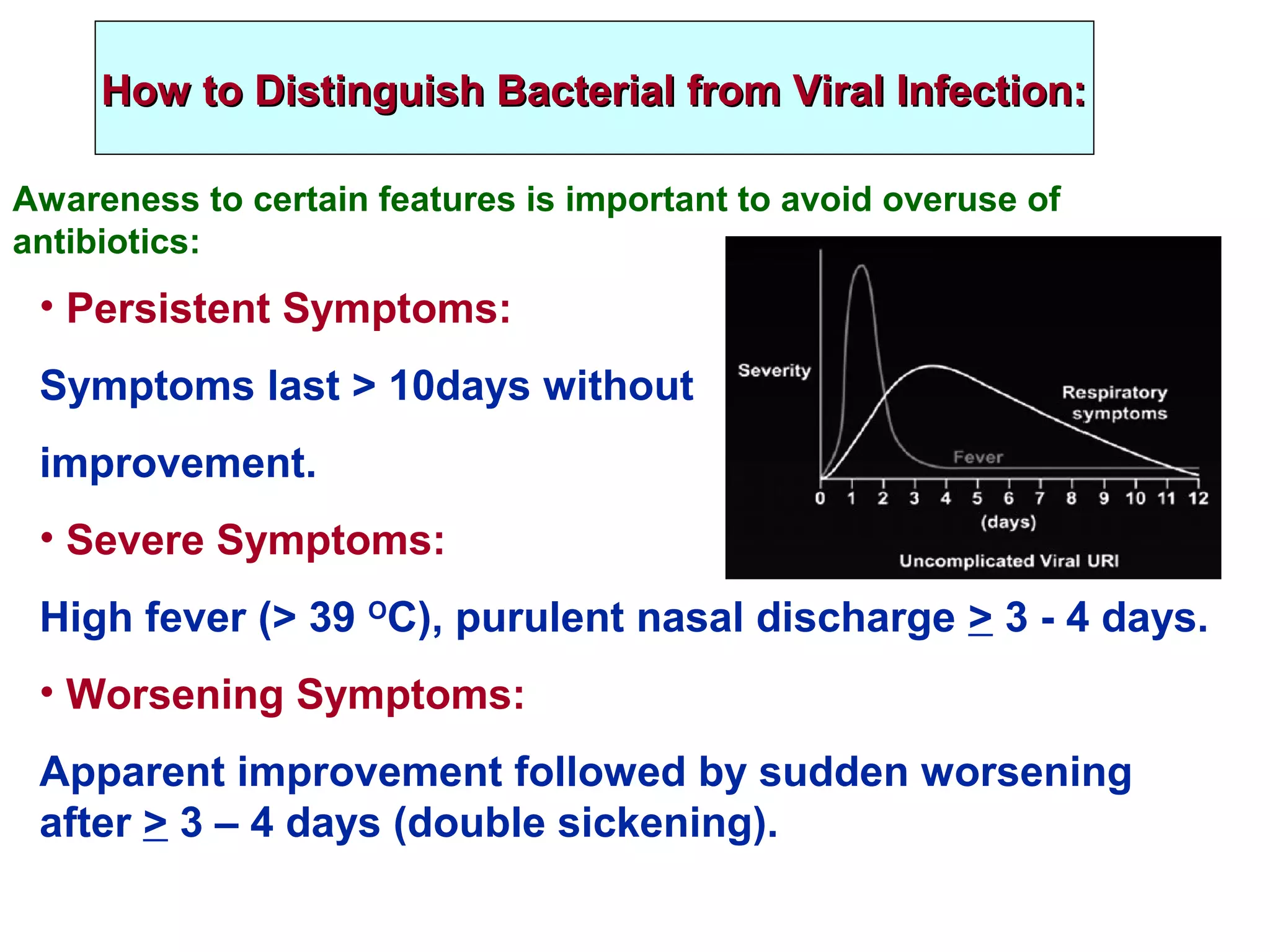
Upper respiratory tract infections are very common and include conditions like sinusitis, ear infections, epiglottitis, and sore throat. While most are mild and viral, inappropriate antibiotic use has led to increased antibiotic resistance. Acute bacterial rhinosinusitis is usually treated with amoxicillin/clavulanic acid for 5-7 days. Chronic rhinosinusitis requires long-term treatment including nasal steroids, saline irrigation, and sometimes antibiotics or surgery. Group A streptococcal pharyngitis is the only commonly occurring sore throat for which antibiotics are indicated to prevent complications like rheumatic fever. A rapid strep test aids early diagnosis and penicillin remains the treatment of choice.