Downloaded 34 times

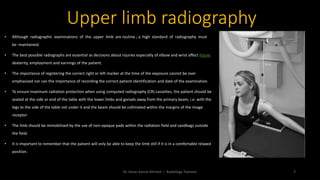

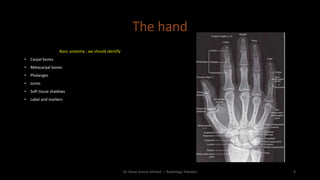
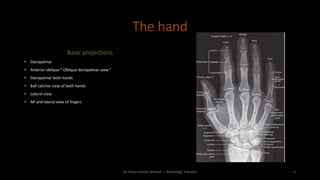
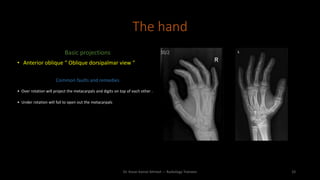
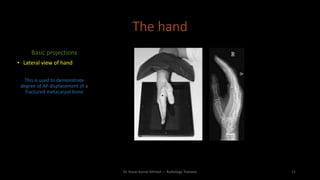
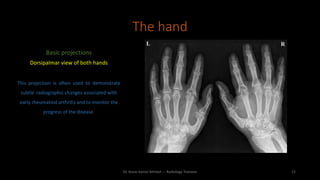
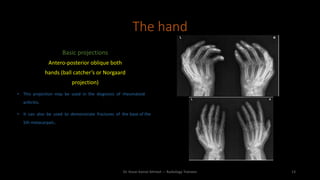
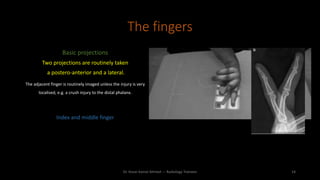

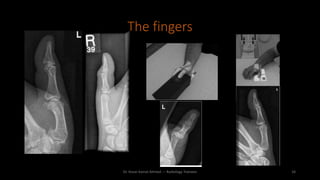




The document discusses guidelines for proper upper limb radiography techniques. It emphasizes maintaining high standards, ensuring correct patient identification and positioning to minimize radiation exposure. Proper hand positioning and identification of anatomical structures is important. Standard projections of the hand include dorsopalmar, oblique, lateral, and views of both hands. Finger projections typically include PA and lateral views. The thumb also requires PA and lateral views. Overall care is needed to obtain clear images while protecting patients.


















































































