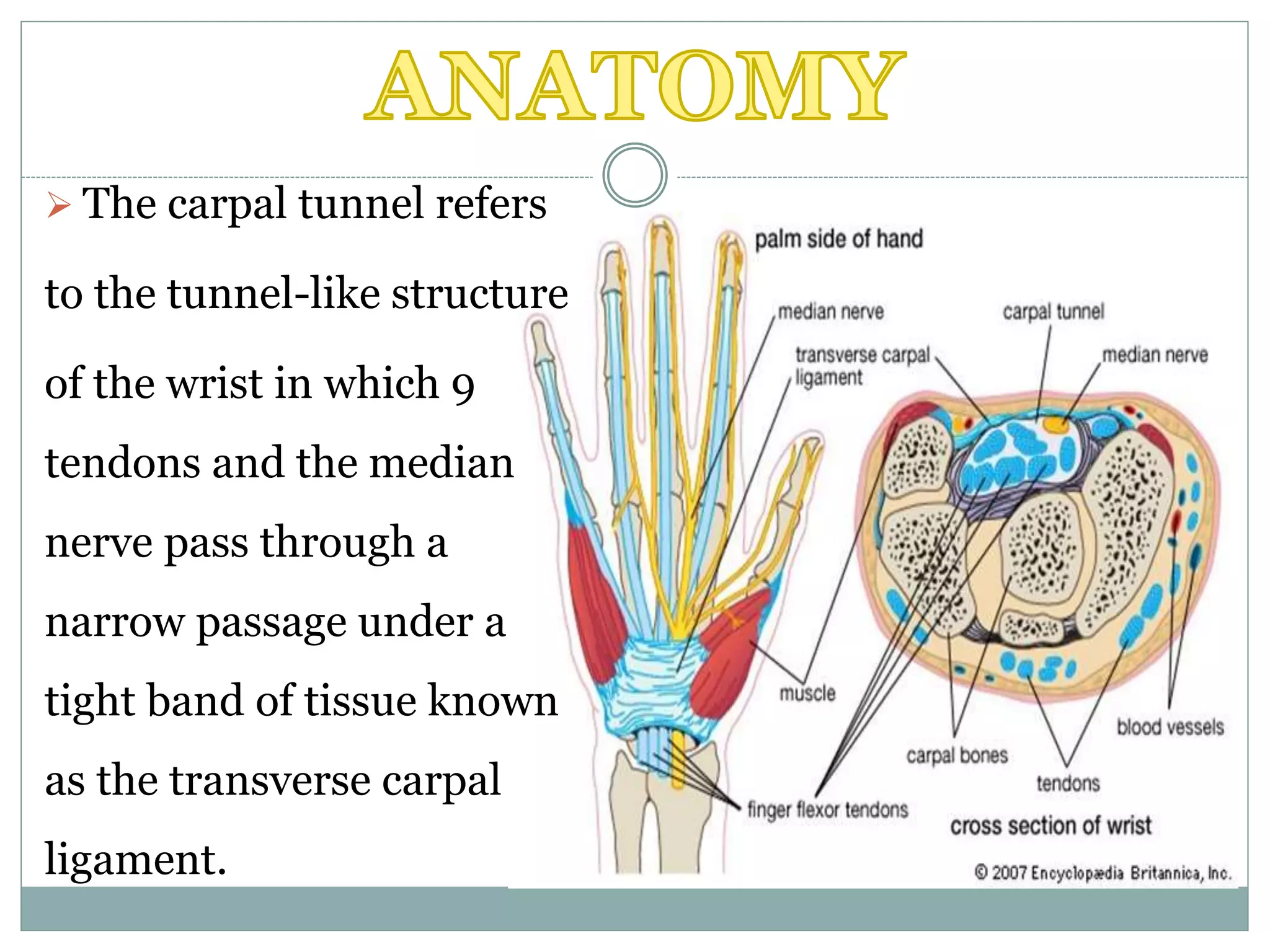
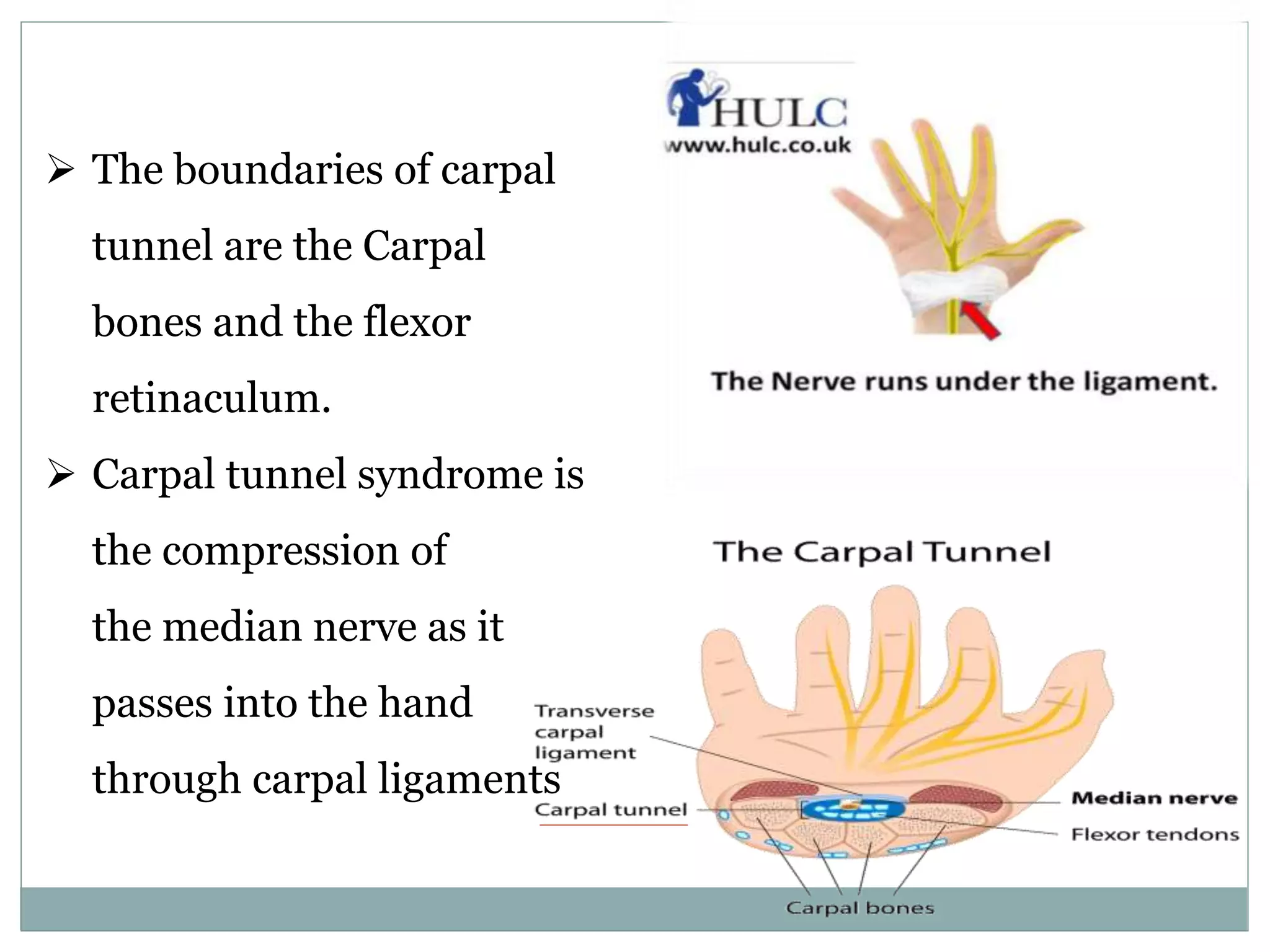
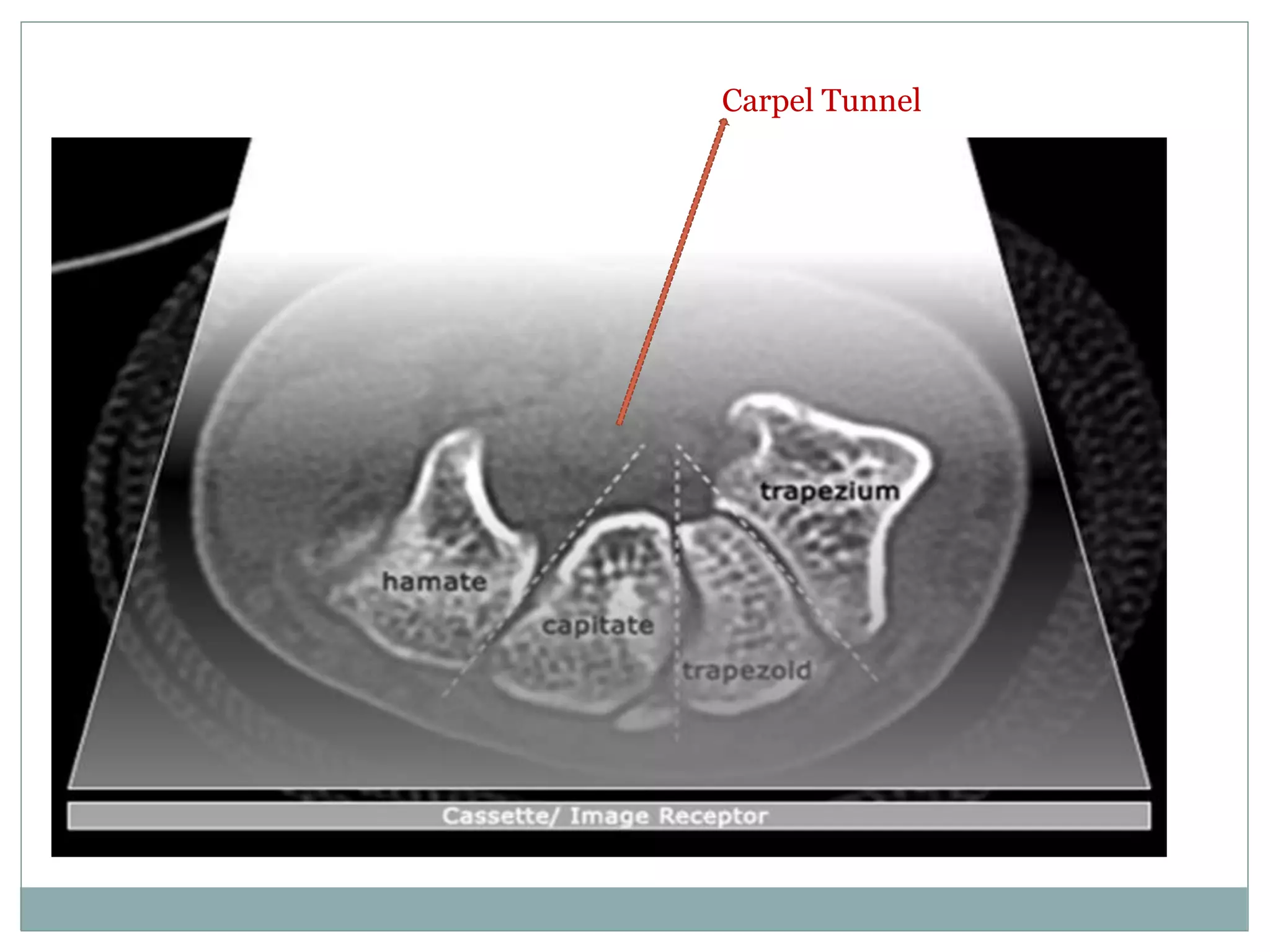
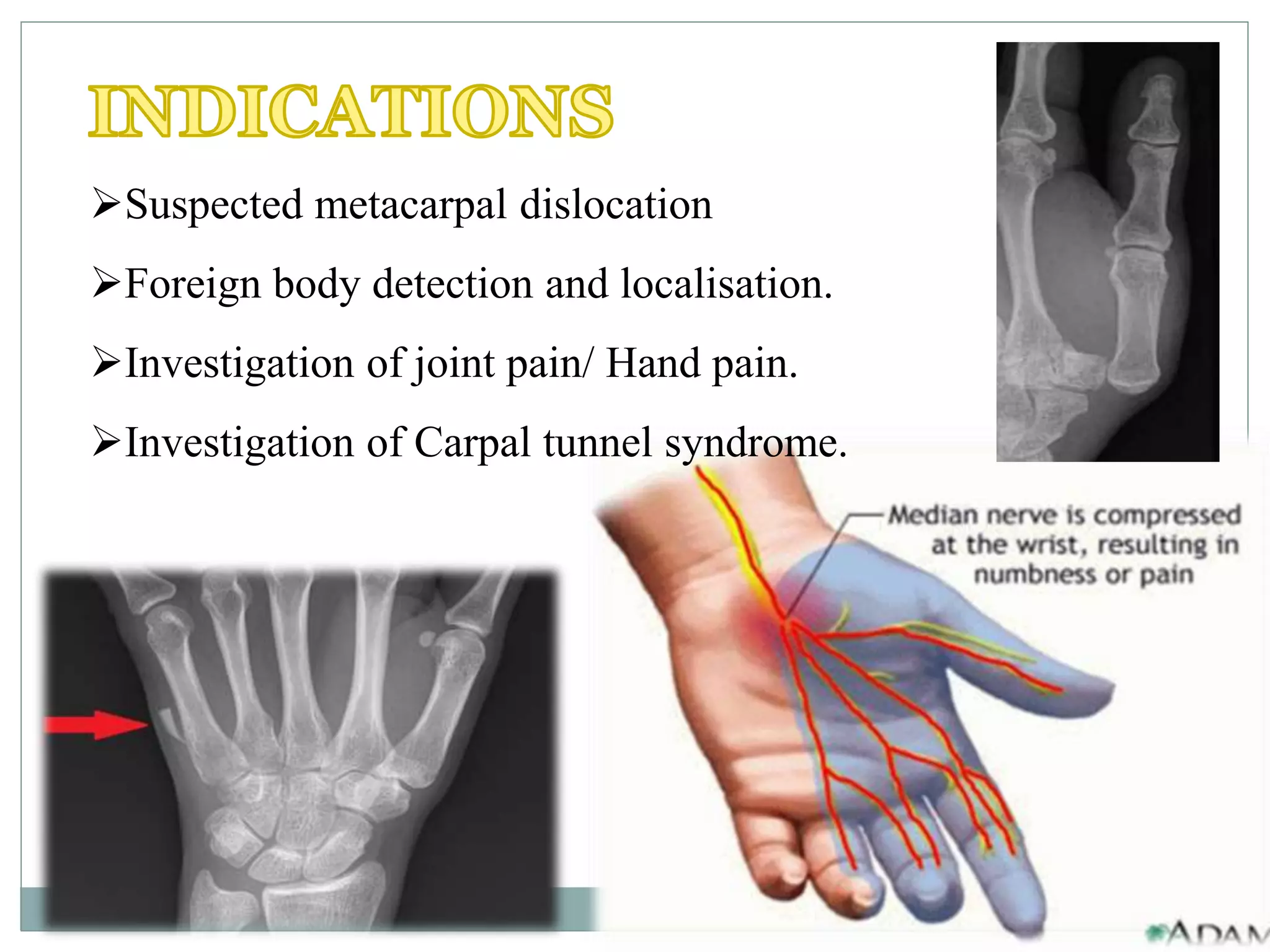
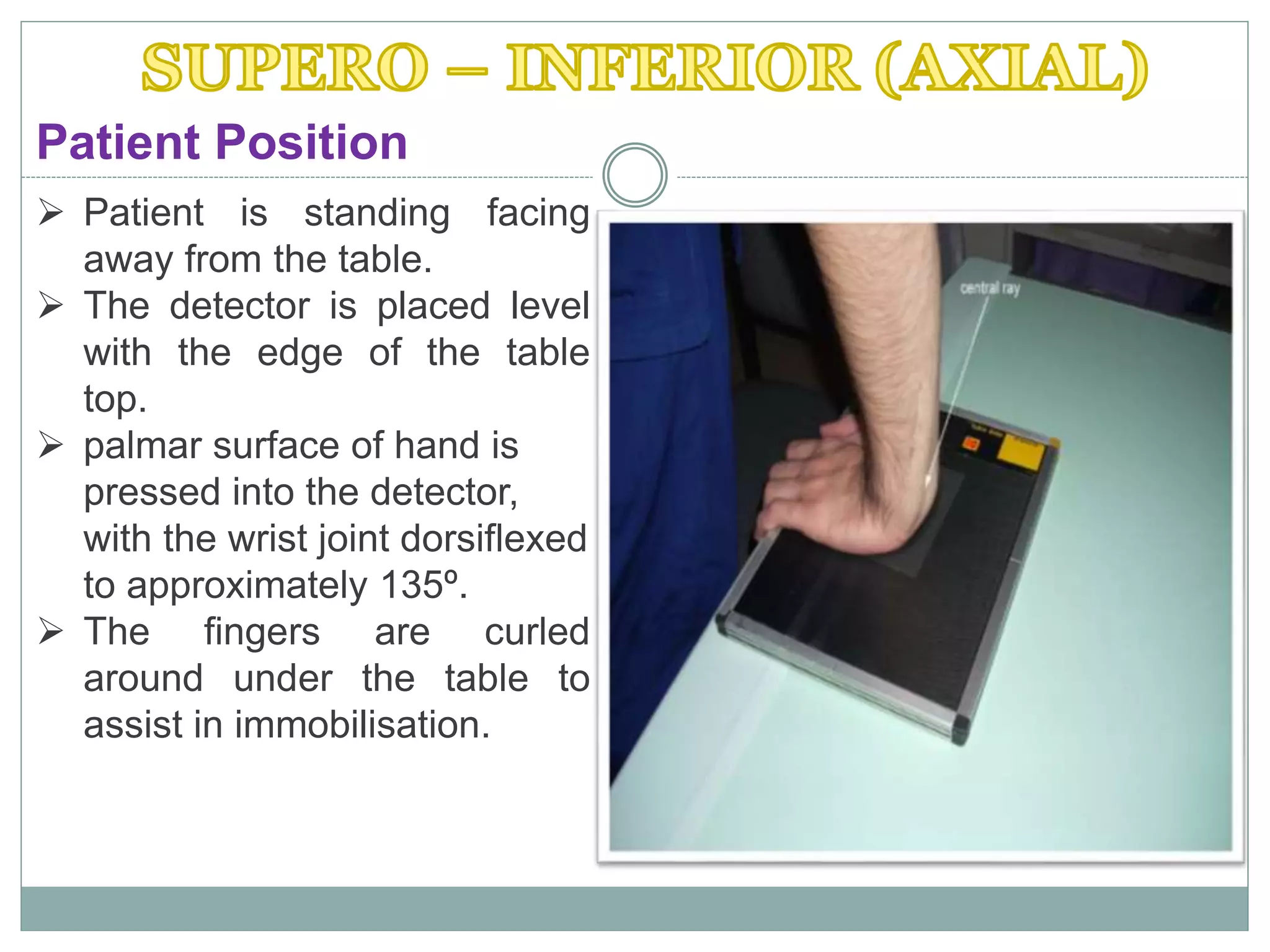
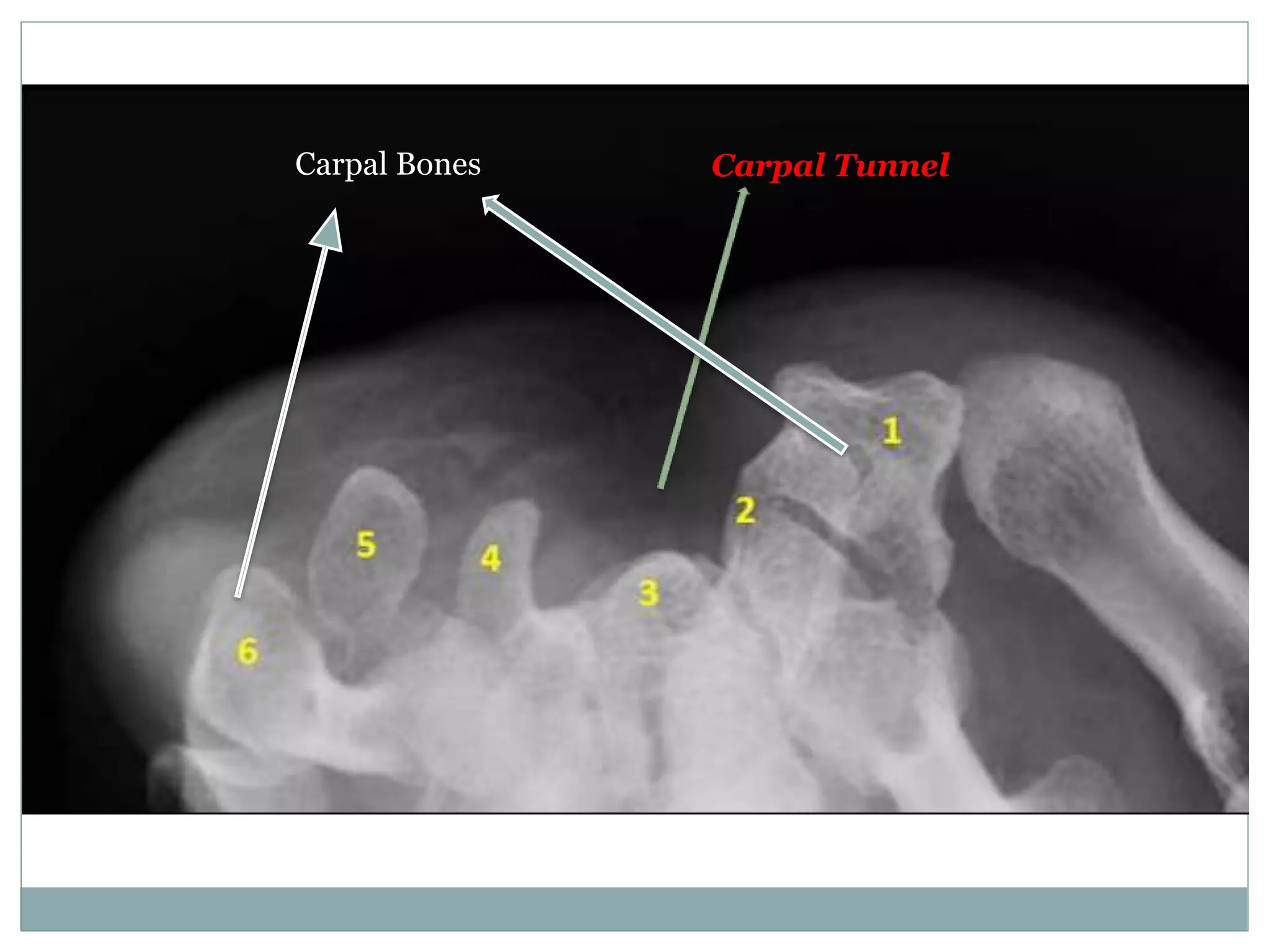
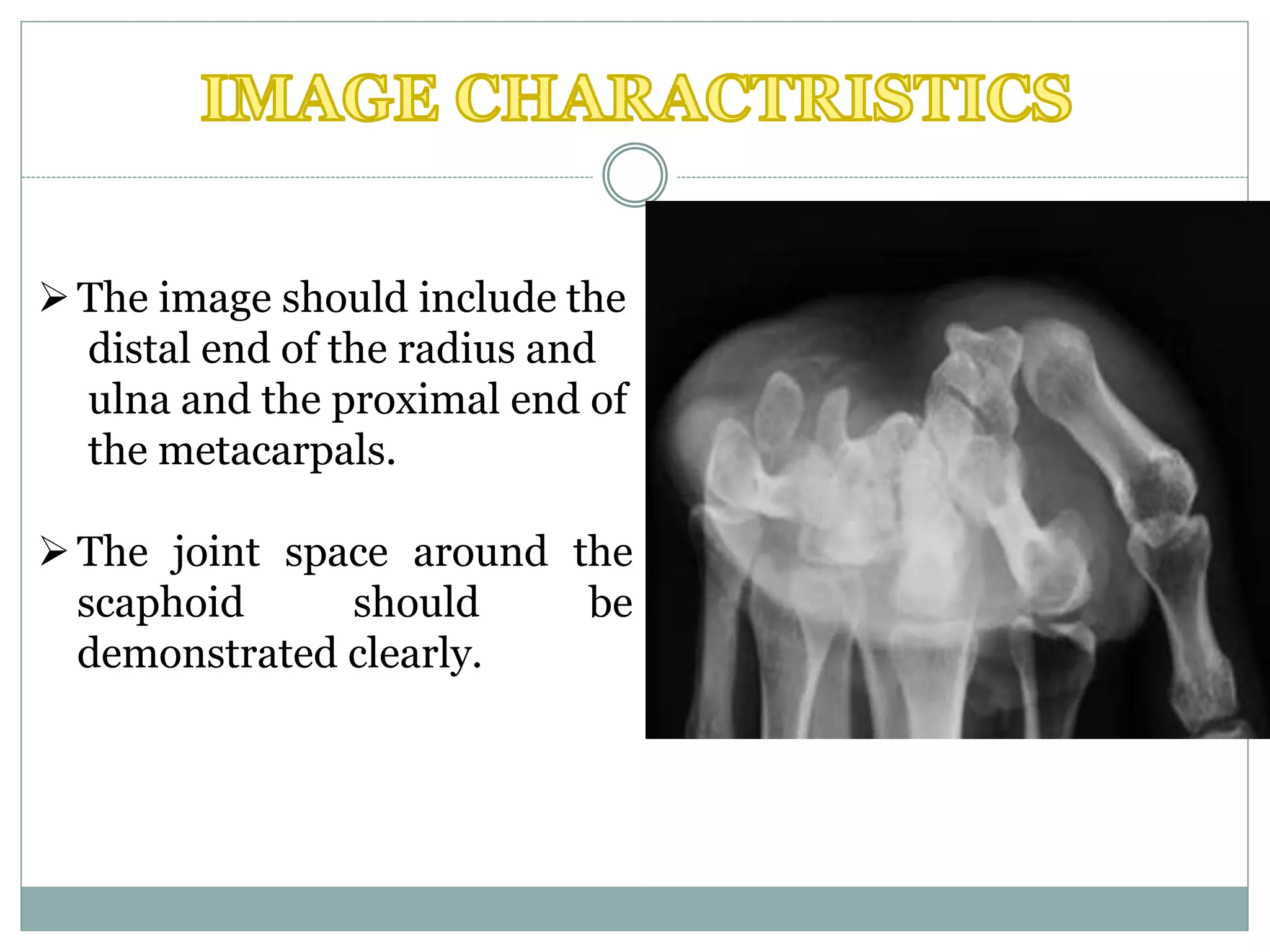
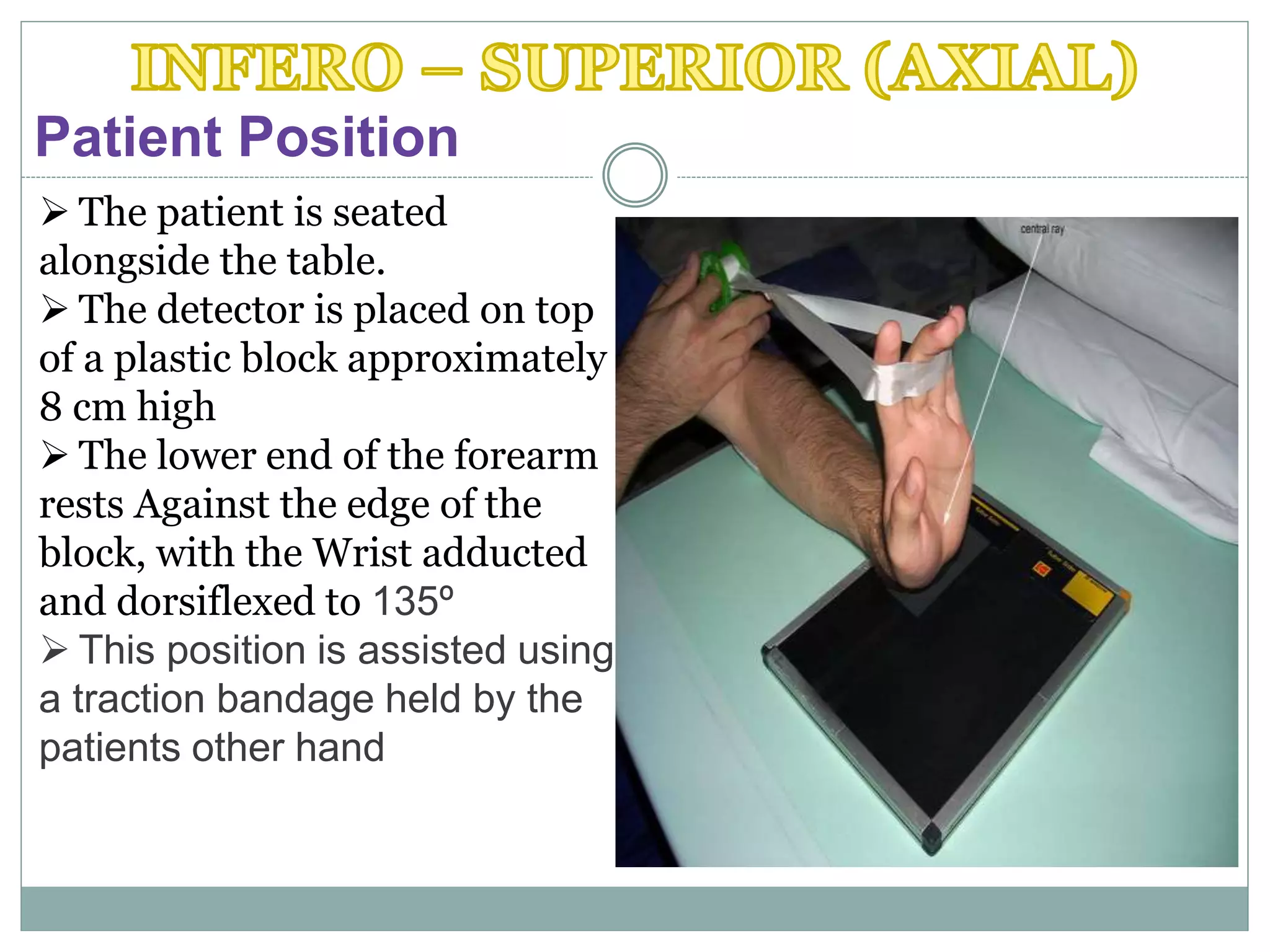
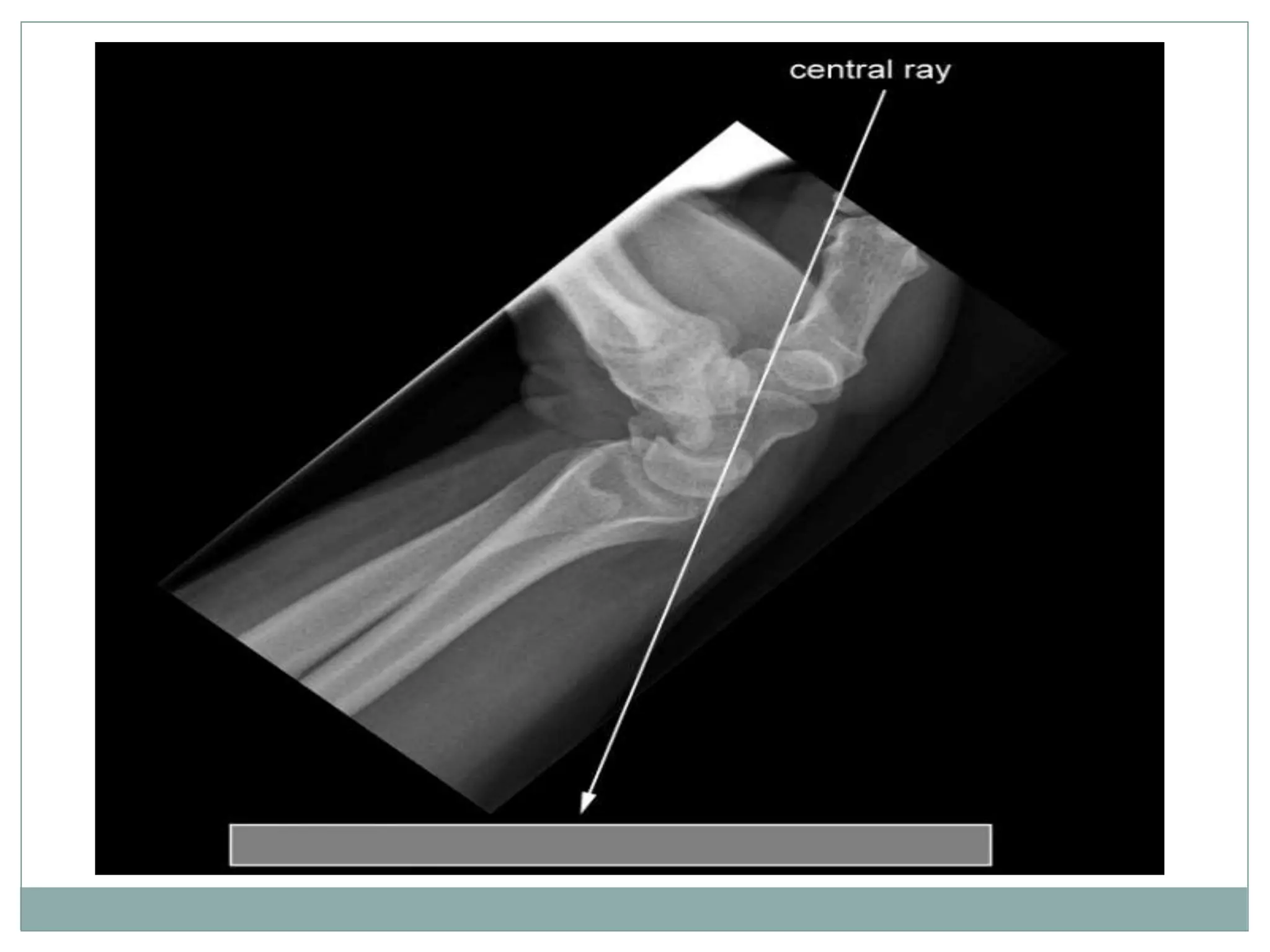
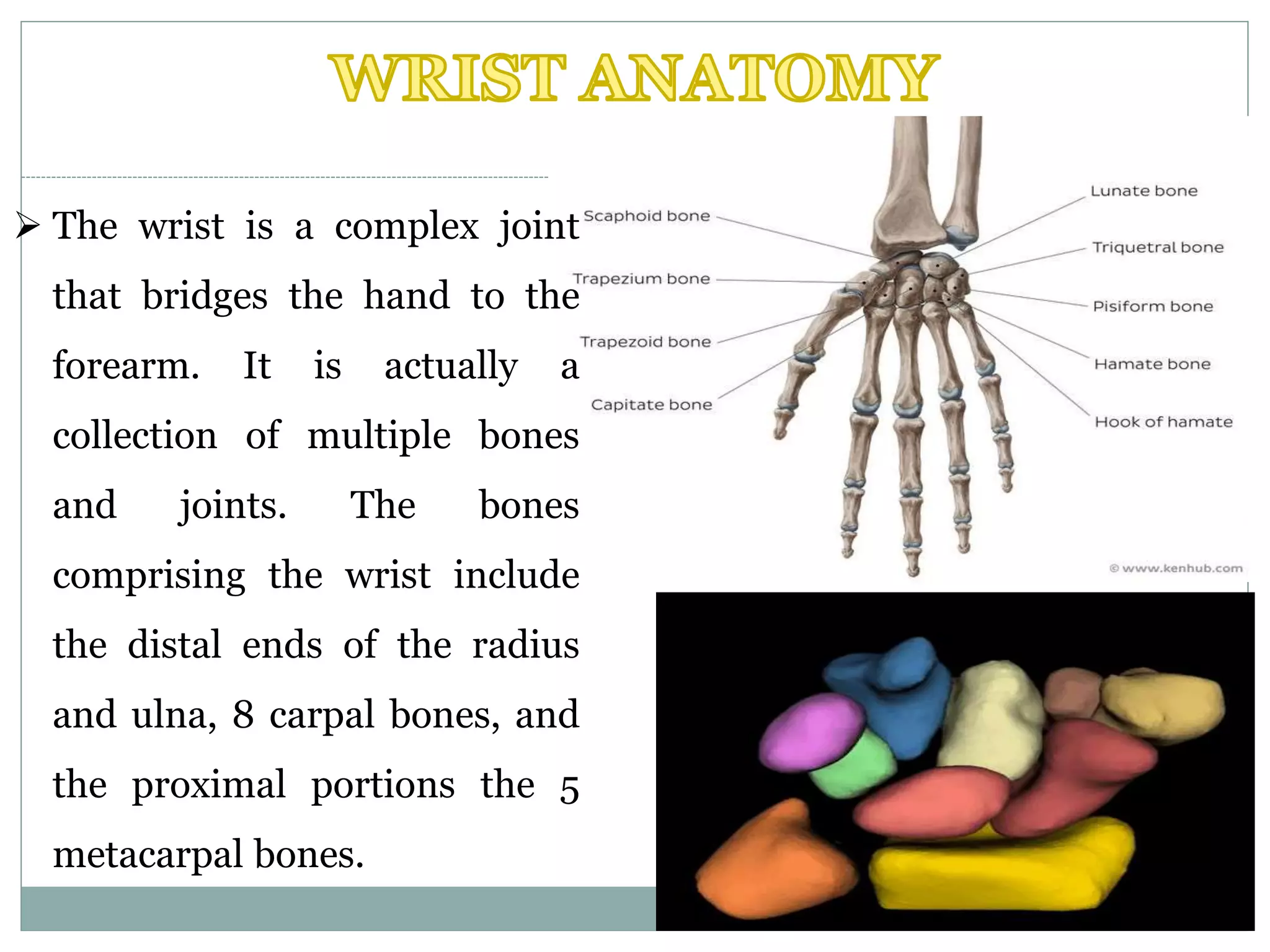
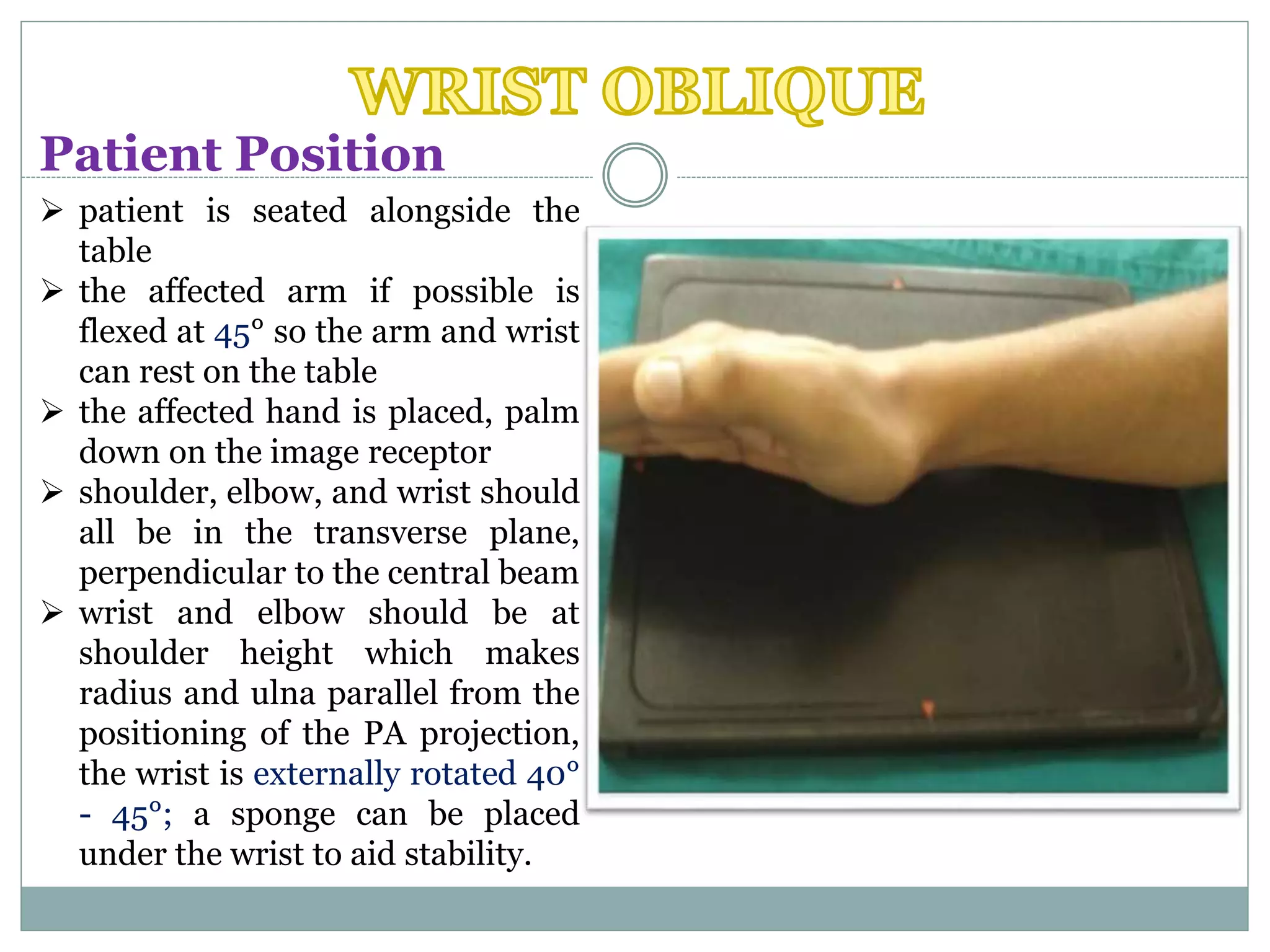
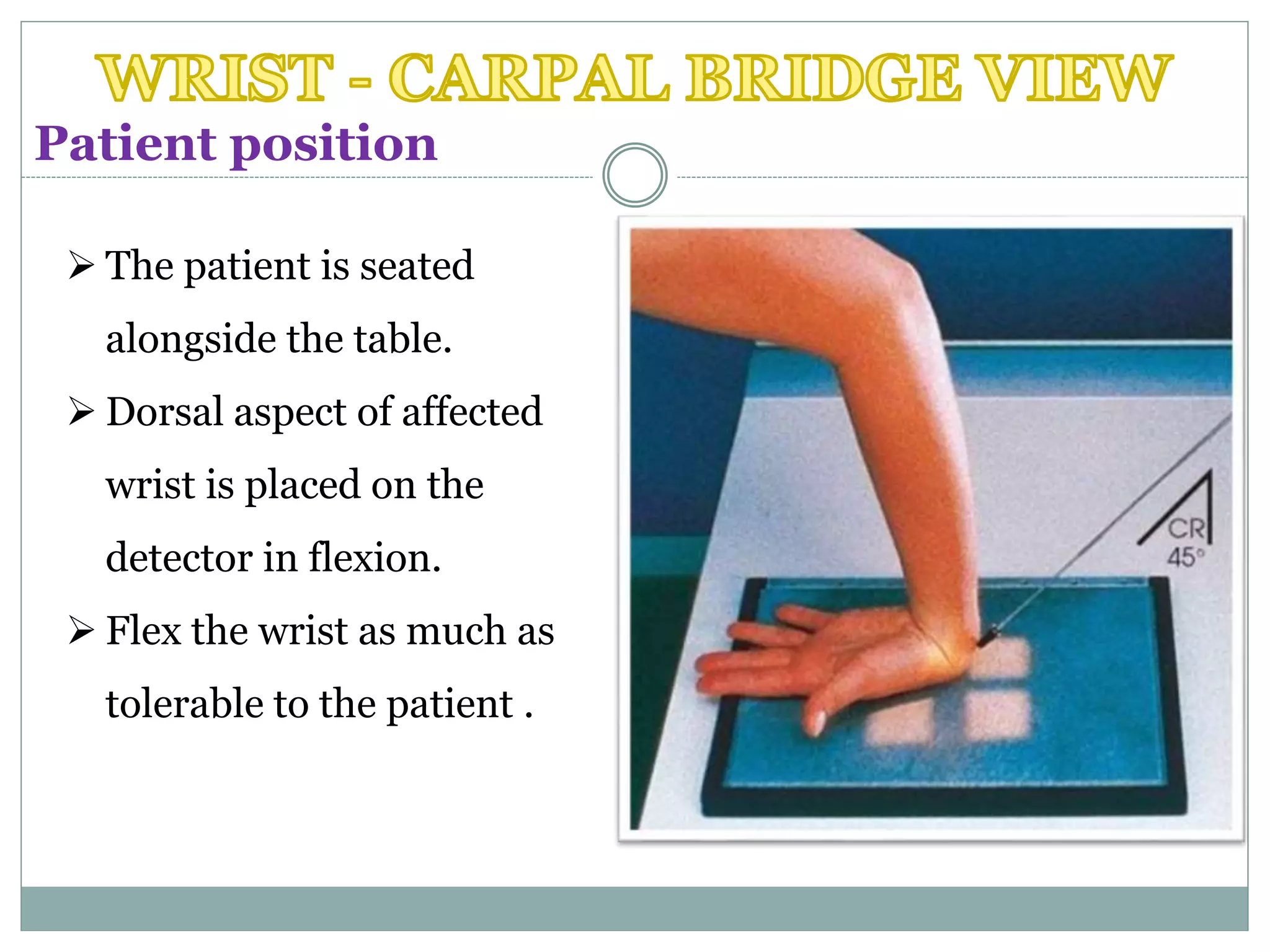
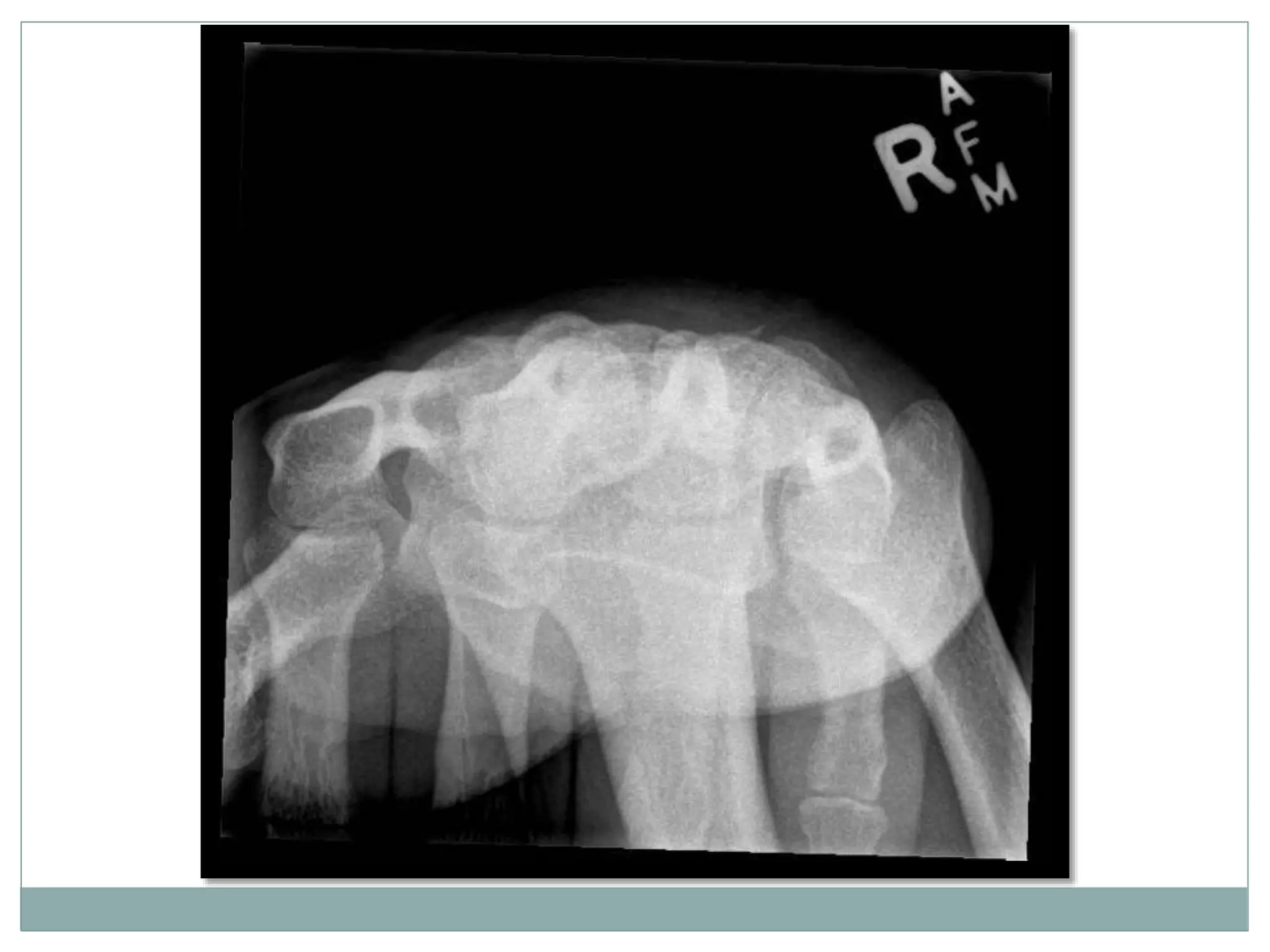
The document provides a detailed overview of the carpal tunnel and its anatomy, focusing on the median nerve and associated syndromes. It outlines various imaging techniques and patient positioning for radiographic assessment of wrist conditions, including carpal tunnel syndrome and fractures. The document emphasizes the complex structure of the wrist, detailing various views and exposure settings necessary for effective imaging.