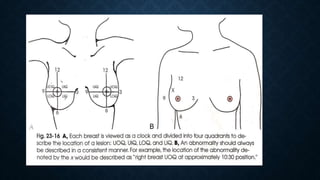
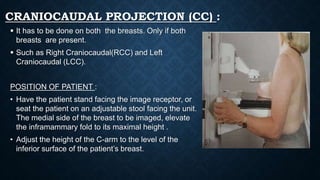
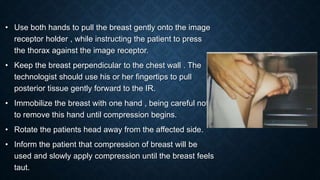
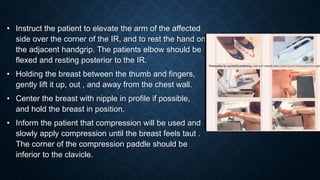
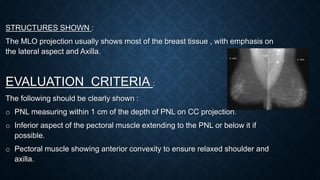
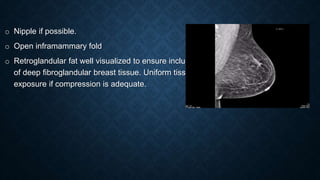
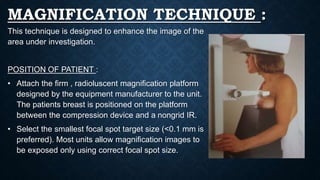
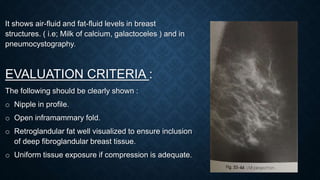
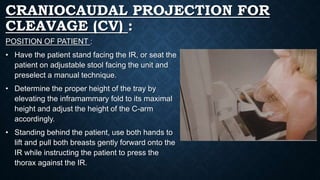
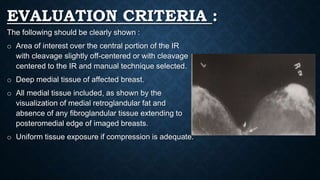
This document provides information about mammography projections and techniques. It begins with the anatomy of the breast and then describes the basic projections used in mammography including craniocaudal, mediolateral oblique, magnification, and others. It explains the positioning of the patient and technical factors for each projection. It also discusses indications for mammography and evaluation criteria for the images. The purpose of the different projections is to visualize different areas of the breast to detect abnormalities. Proper technique is important for high quality images.