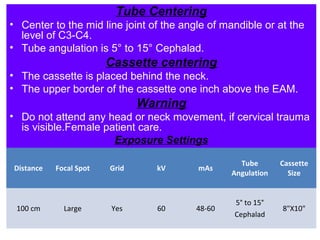
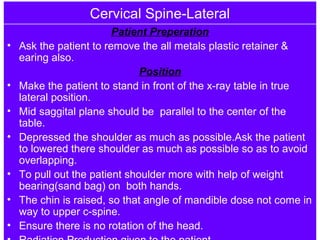
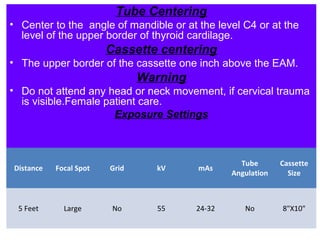
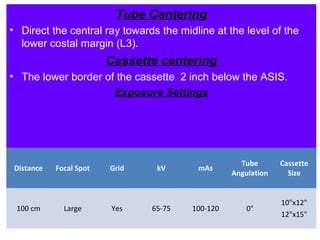
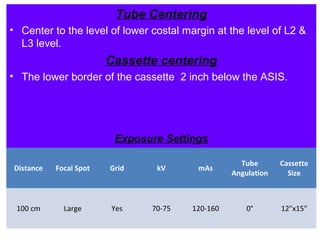
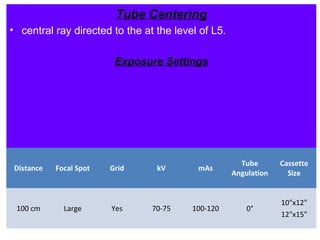
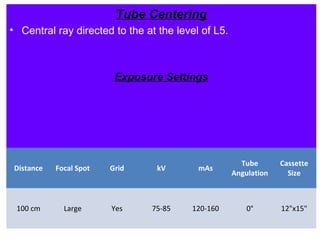
This document provides positioning guidelines for radiographic imaging of the cervical spine, thoracic spine, lumbar spine, lumbo-sacral spine, and sacrum. It describes the standard views, patient preparation, positioning, tube and cassette centering, and exposure settings for each anatomical region. Proper patient positioning and radiographic technique are important to obtain diagnostic images while minimizing radiation dose.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









