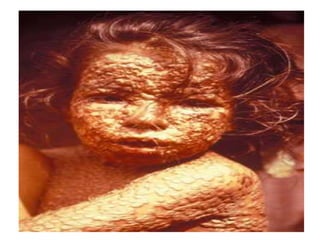
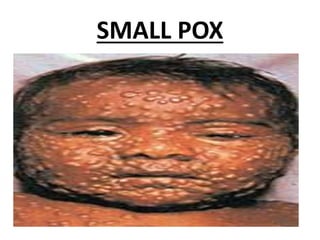
The document summarizes India's immunization programme and history. It discusses how Edward Jenner developed the smallpox vaccine in 1796, leading to smallpox eradication globally by 1977. India launched its Expanded Programme on Immunization in 1978 to provide vaccines for 6 diseases to children under 5 and pregnant women. This programme evolved into the Universal Immunization Programme in 1985 to achieve universal immunization coverage across the country. Significant milestones and achievements of India's immunization efforts are highlighted.





































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)












