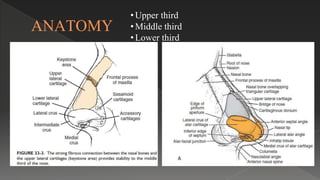
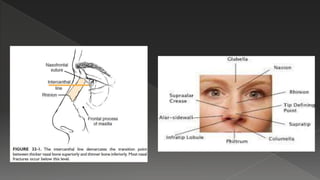
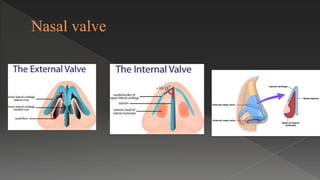
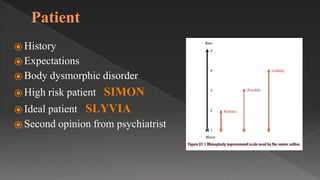
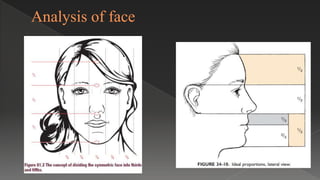
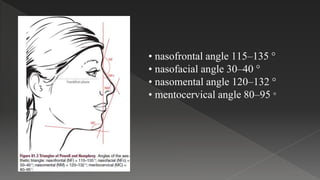
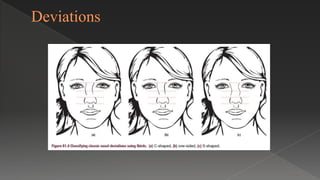
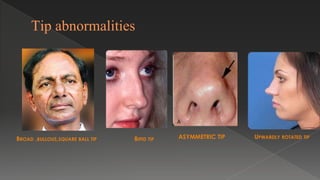
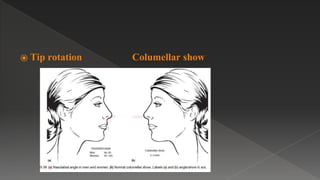
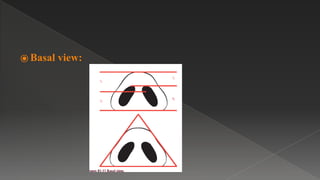
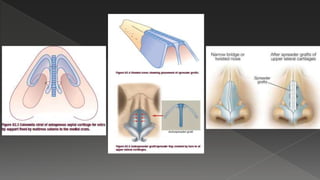
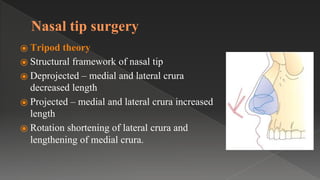
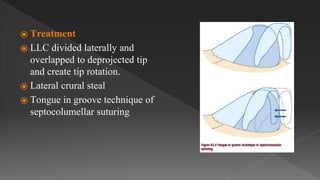
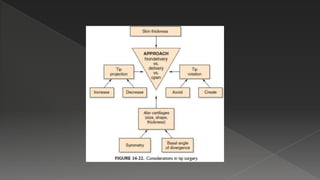
Rhinoplasty is a challenging facial plastic surgery procedure. The nose is divided into thirds for analysis - upper, middle, and lower. Preoperative assessment considers facial aesthetics, nasal function, and patient expectations. Analysis of the nose includes inspection of external and internal structures as well as palpation. Deviations, tip abnormalities, and alar issues are evaluated. Rhinoplasty techniques can be open or closed. Specific structures like the nasal bones, septum, and nasal tip are addressed through techniques like osteotomies and structural framework modification. Grafting materials are used for augmentation and to correct deformities. Potential complications are addressed.