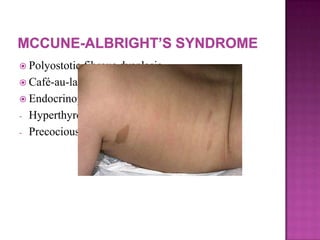
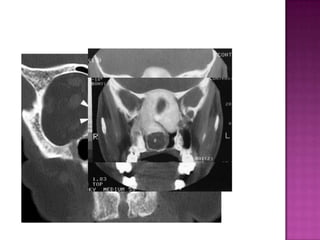
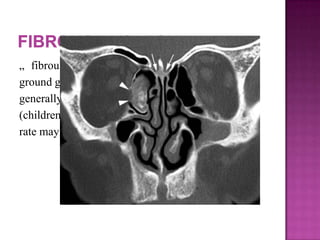
This document discusses various fibro-osseous tumors of the sinonasal region, including fibrous dysplasia. Fibrous dysplasia is a benign condition caused by a defect in osteoblast differentiation and maturation, resulting in the replacement of normal bone by fibrous connective tissue. It is caused by mutations in the GNAS1 gene. Histologically, there is slow replacement of medullary bone by abnormal fibrous tissue at different stages of bone metaplasia. Fibrous dysplasia typically presents in children and adolescents, with females being affected more often than males.
![ Kamel et al. Type 1: Tumour originating from the
nasal septum or lateral nasal wall.
Type 2: Tumour originating from the maxillary
sinus.
[This classification focuses on origin and not size /
extent of tumour-does not analyze frontal sinus
separately]](https://image.slidesharecdn.com/benignsinonasalmasses-presentationmanagement-1-130928125330-phpapp01/85/Benign-sinonasal-masses-presentation-management-1-26-320.jpg)