1. The nasal tip's support structures include bone, cartilage, and soft tissue attachments between these structures.
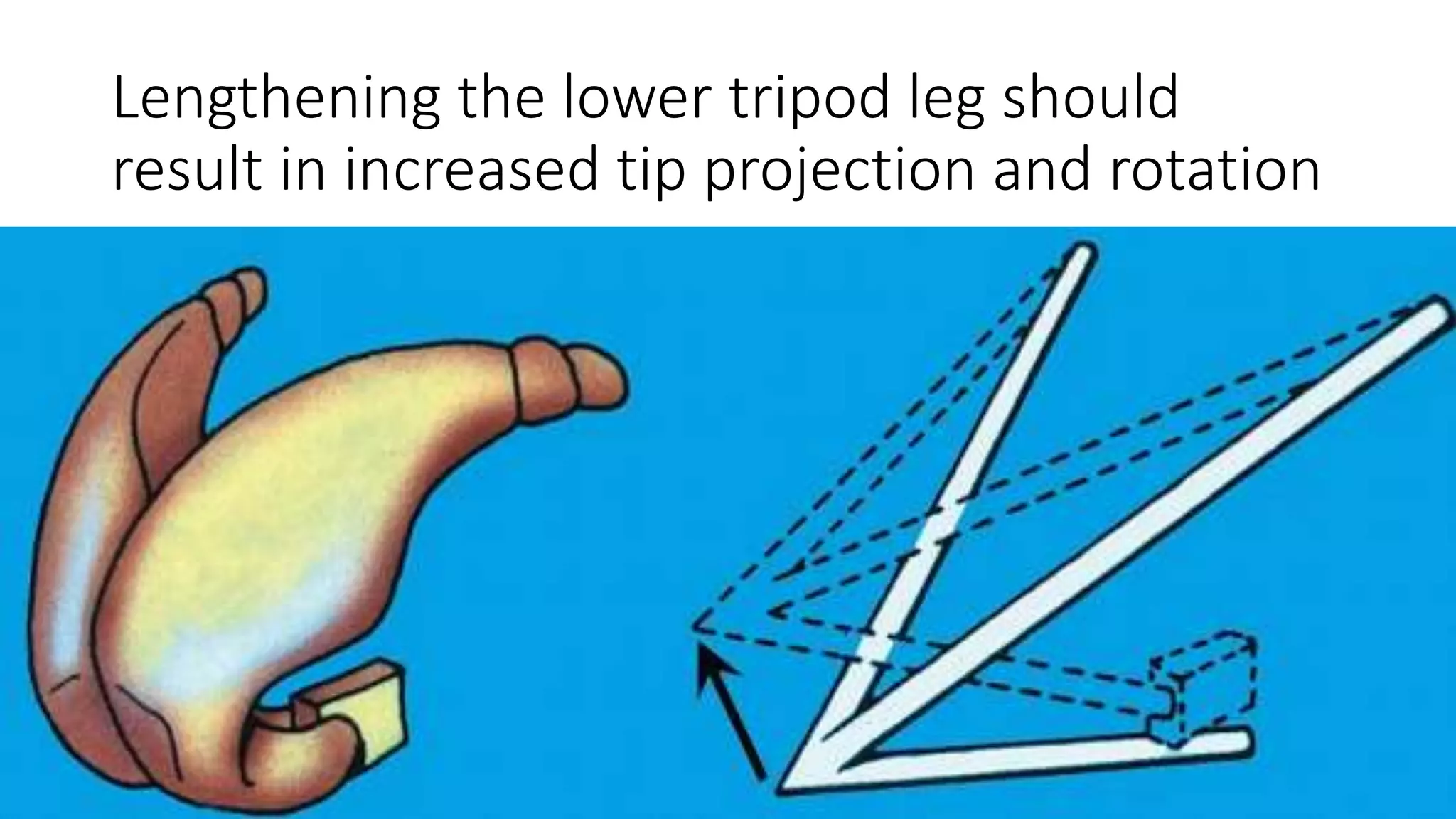
2. Modifying the nasal tip cartilages and related structures can alter the tip's projection, rotation, and definition.
3. Various surgical techniques can be used to increase or decrease tip projection and rotation, including modifying the lateral and medial crural attachments and using grafts. Precise suturing techniques are also important for shaping the tip.