Download to read offline



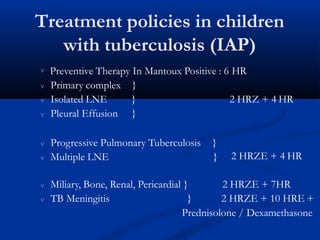

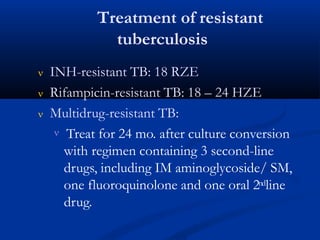
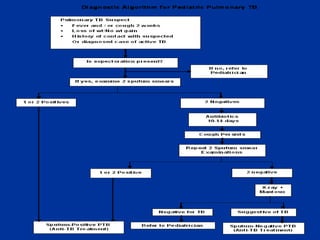

This document summarizes childhood tuberculosis. It begins by defining tuberculosis and describing the portal of entry and primary infection. It then discusses the clinical states that can arise from TB infection in children versus adults. The rest of the document details various forms of TB based on organ system affected, along with their associated symptoms, presentations and complications. Radiological findings are also described. The diagnosis, treatment and policies for childhood TB are outlined.























































