Download as PDF, PPTX

![Issues: CKD Vit D products (eg calcitriol)
A) Ca/PO4 metabolism in CKD - give if iPTH >21 or 3x normal upper limit
- contraindications: Ca- PO4 >55, PO4 >2.0 or iPTH <15 (as further suppression of iPTH
by Vit D will cause impaired bone remodeling and higher risk of fractures
Decreased renal Decreased Acidosis secondary to - monitoring of iPTH – ideally, yearly in stage 3, half yrly in stage 4, 4-6 mthly in stage 5
excretion of PO4 renal mass
+
decreased H excretion 4) Secondary hyperparathyroidism due to hyperplasia of parathyroid gland
iPTH usually >100
perform U/S or Sestamibi scan to locate PTH glds, as there may be >4. Sestamibi scan
preferred
Decreased Rx: surgical removal +/- partial reimplantation of portion of PTH gland
hydroxylation of Vit D 5) Treating hypocalcaemia
Decreased GI IV Ca Gluconate contains 2.4mmol/10ml, IV CaCl2 contains 7 mmol/10ml of calcium
Ca absorption ions
Higher risk of phlebitis with CaCl2, and also, more severe in event of extravasation.
Always give CaCl2 intra-hemodialysis, via central line, or at least via large bore cannula
Decreased if possible, unless in event of emergency.
serum Ca
Increased bone B) Anaemia in CKD
Increased iPTH osteoclastic activity Causes LVH and increase risk of cardiovascular disease
secretion Ideal target 11-11.5 g/dL, however locally, usually aim for 8g/dL in view of Rx costs.
(Note: Hb > 12.5 also a/w increased mortality)
iPTH/PO4 Work up:
iPTH and PO4 levels start rising o Fe panel – Ferritin <200 + Tsat <20% = Fe deficiency in hemodialysis
exponentially from CKD stage 3 (in peritoneal dialysis, limit for ferritin is <100)
increased PO4 levels correlates to greater Tsat = transferrin saturation = Fe ÷ transferring x100%
cardiovascular risk o Vit B12/folate
o PBF
o OGD
o +/- stool OB
Mx 1 2 3 4 5 Mx
1) Diet – first line Fe Fumarate – 400-800mg/day, give on empty stomach (eg ON)
- limit PO4 intake to 800mg/day (dietician r/v) IV venofer 100mg x 8-10 doses. CI: Ferritin >500 or Tsat >50%
2) Phosphate binders Erythropoeitin
i) CaCO3 - higher elemental Ca load, & better tasting. Therefore better for o Start if Hb <10-11. Starting dose 100unit/kg/wk (eg 6000U/wk).
calcium supplementation Monitor for 3-4 wks before increasing dose as necessary.
ii) Ca Acetate – higher phosphate binding capacity, but large and bad tasting. o Max 30,000 U/wk
Better for managing high phosphate levels o If poor response, consider possible causes
iii) MgSO4 – bad tasting, risk of Mg toxicity. Common SE of diarrhea Inflammation/infection (raised ferritin)
iv) Al(OH)3 – risk of aluminium toxicity (eg poor BP ctrl, encephalopathy), not for Malnutrition (low albumin)
use for >6wks. Secondary hyperparathyroidism
v) Seralamer – amino acid polymer. Gd for ctrl of acidosis as well, but expensive Malignancy
vi) Dialysis Aluminium toxicity
Give CaCO3/ Ca acetate between meals if trying to supplement Ca. Give with meals if ACE/ARB
trying to bind phosphate. Insufficient dialysis
Calcium-phosphate binding product = [Ca] x [PO4] Pure red cell aplasia (rare)
- if >55 (calculations in mmol), OR if [Ca] 2.50 mmol/L, avoid Ca based phosphate
binders in view of risk of metastatic calcium product deposition
Targets: CKD Stage 3-4 keep [PO4] <1.5; Stage 5 keep [PO4] <1.8
Low phosphate levels also indicate likely malnutrition, as PO4 is found in high protein
Digitally signed by DR WANA HLA SHWE
DN: cn=DR WANA HLA SHWE, c=MY,
food o=UCSI University, School of Medicine, KT-
Campus, Terengganu, ou=Internal Medicine
3) Calcium supplementation Group, email=wunna.hlashwe@gmail.com
Reason: This document is for UCSI year 4
CaCO3/ Ca acetate between meals students.
Date: 2009.02.22 15:45:33 +08'00'](https://image.slidesharecdn.com/chronicrenalfailureconciselongcaseapproachcrfwithfluidoverloadmxpathway-120907121357-phpapp01/75/Chronic-renal-failure-concise-long-case-approach-crf-with-fluid-overload-mx-pathway-3-2048.jpg)
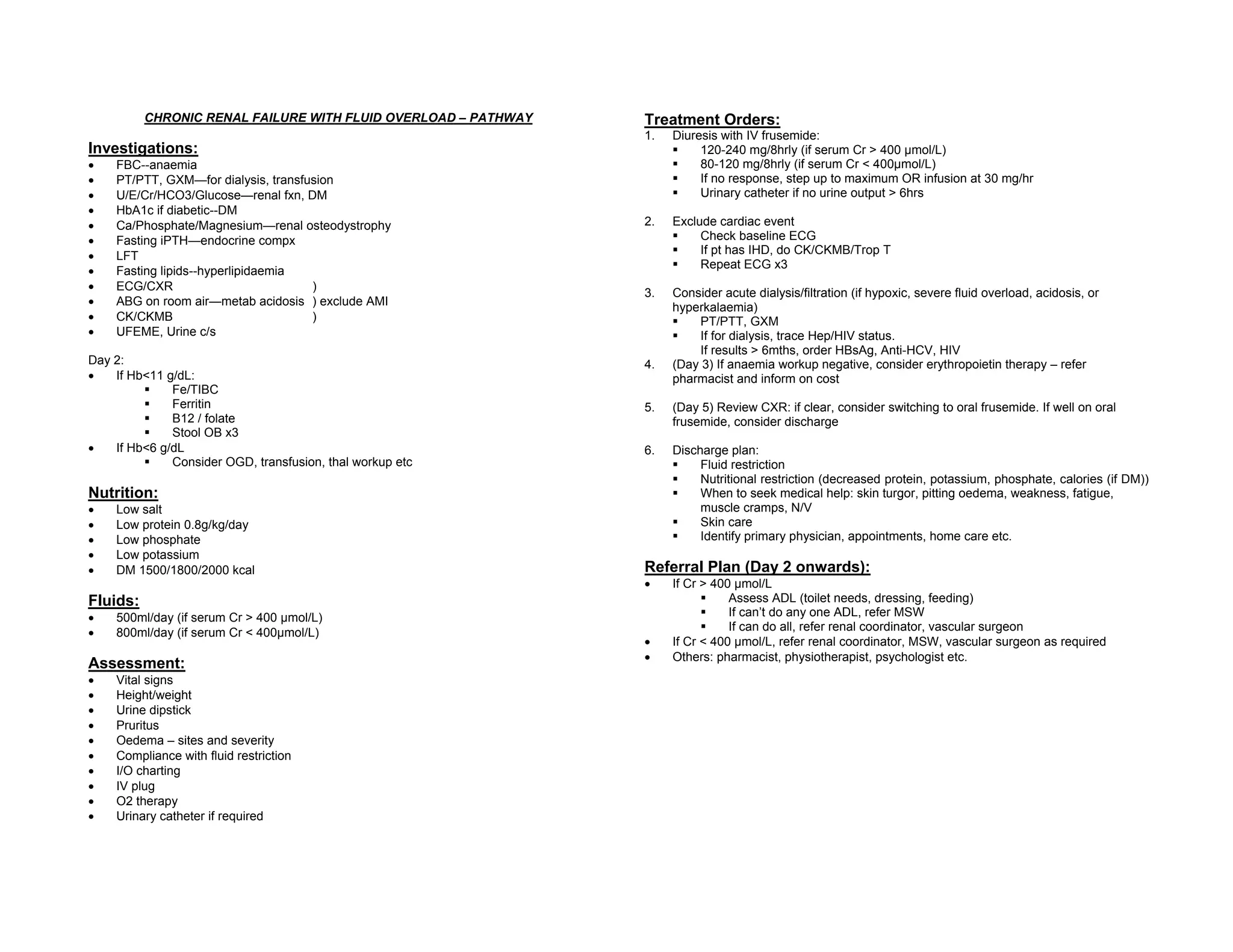

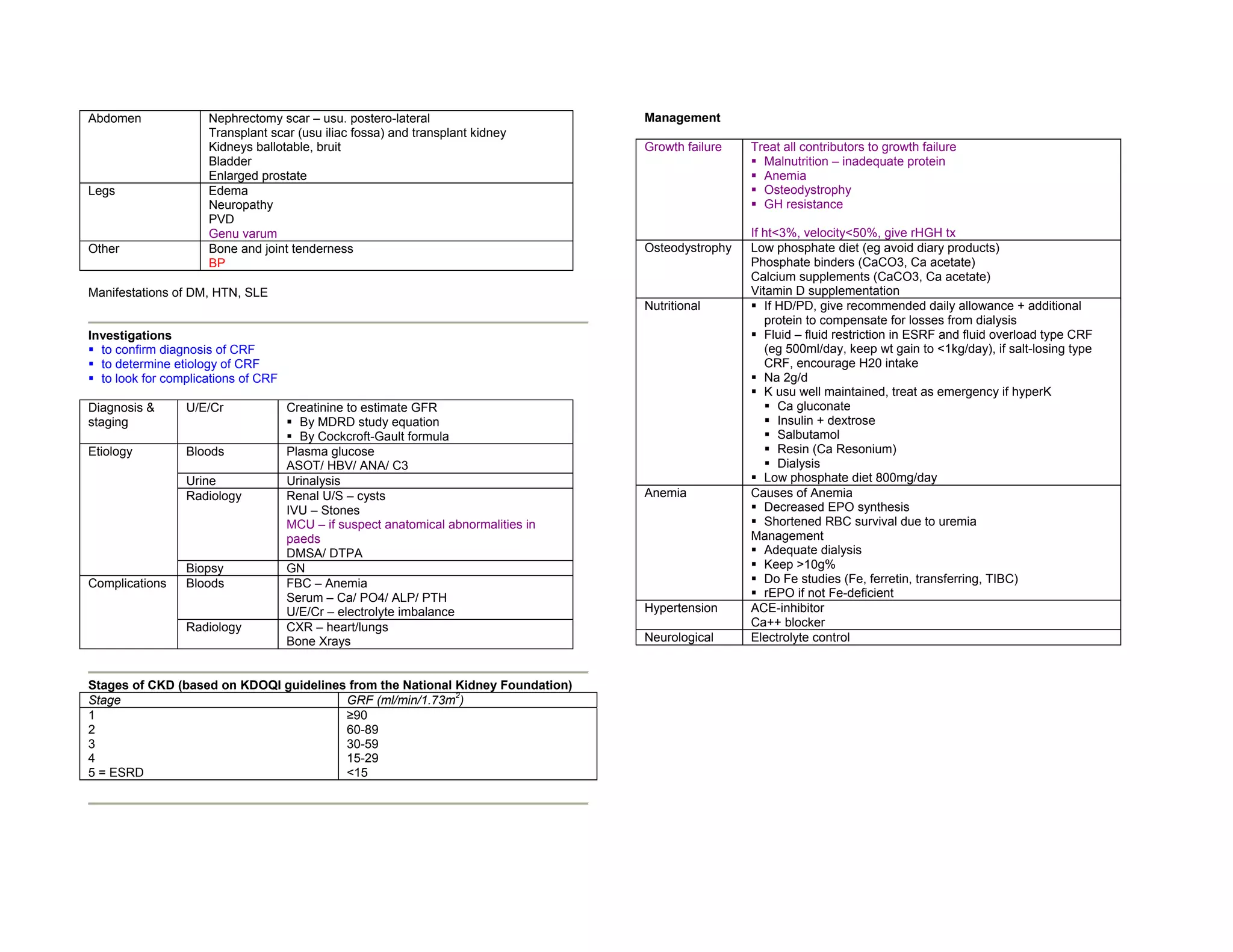
This document provides a concise long case approach for chronic renal failure. It outlines the key presenting complaints, history, physical exam findings, investigations, complications, and management strategies for chronic renal failure. The management involves addressing issues related to calcium/phosphate metabolism, anemia, osteodystrophy, fluid overload, and nutritional management. Treatment plans include diuresis, dialysis/filtration, erythropoietin therapy, calcium supplementation, and dietary restrictions. Referrals to other specialists are recommended based on the severity of renal failure and patient needs.























































































