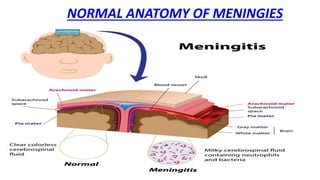
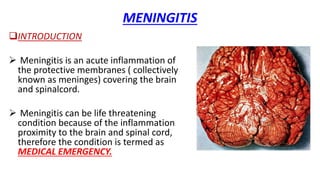
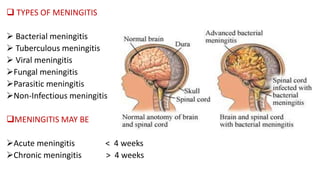
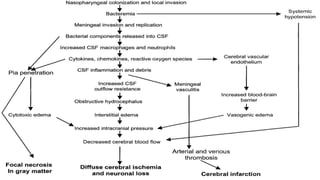
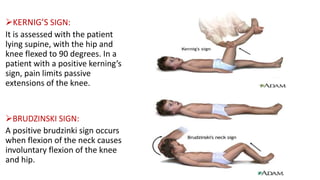
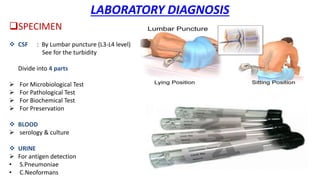
This document discusses common central nervous system (CNS) infections including meningitis, encephalitis, and brain abscess. It provides information on the causative organisms, pathogenesis, signs and symptoms, and laboratory diagnosis of bacterial, viral, fungal and parasitic meningitis. It also discusses meningitis cases, the anatomy of the meninges, and complications of meningitis. Encephalitis and brain abscess are also summarized, including their causes, pathogenesis, clinical features and diagnostic workup.