Download to read offline

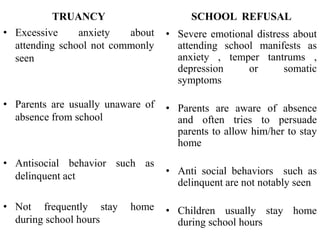













This document discusses truancy, which is when a school-aged child frequently misses school without an excuse. Truancy can be caused by factors related to the child, parents, or school and can lead to conduct problems, low academic achievement, and involvement in criminal behavior. The document outlines approaches for assessing and managing truancy through cognitive behavioral therapy, educational support, pharmacotherapy, and collaborating with parents and teachers. Prevention emphasizes addressing underlying issues through a multifaceted approach involving the school, parents, and child.
















































































