Downloaded 10 times
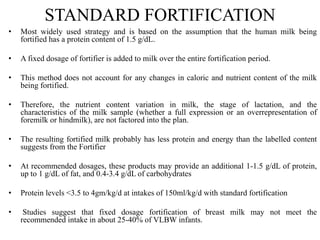

Human milk fortifiers are products that can be added to expressed breast milk to increase its nutritional content for premature infants. There are three main approaches to fortification - standard fixed dosage, adjustable based on blood urea nitrogen levels, and targeted fortification using human milk analysis. Fortifiers provide additional protein, calories, and minerals to help premature infants achieve adequate growth. While fortification benefits growth, high osmolality from fortifiers can cause feed intolerance and risks like necrotizing enterocolitis. Careful monitoring of infants on fortified breast milk is needed to optimize nutrition and growth.
















































































