Download as PDF, PPTX








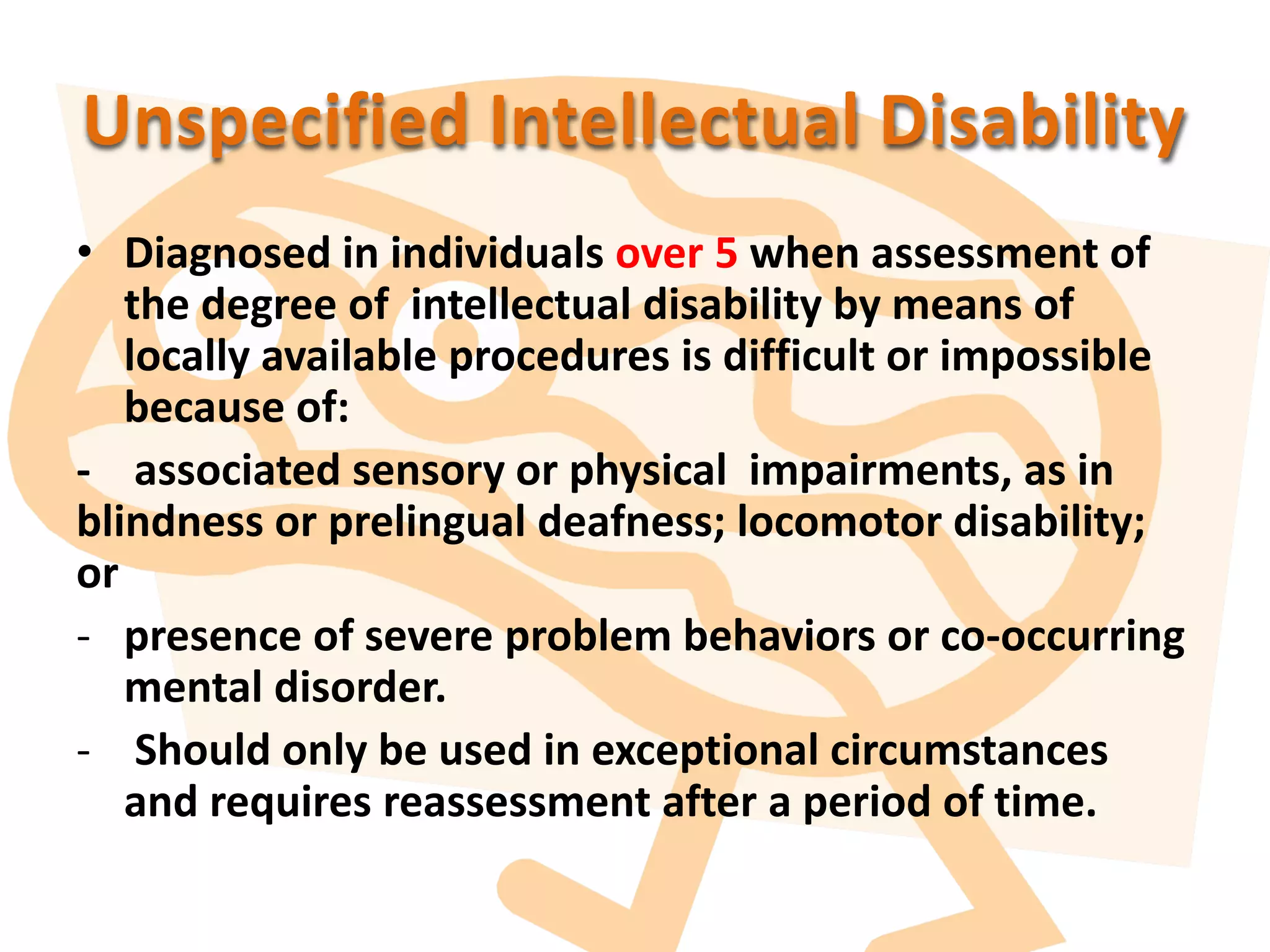
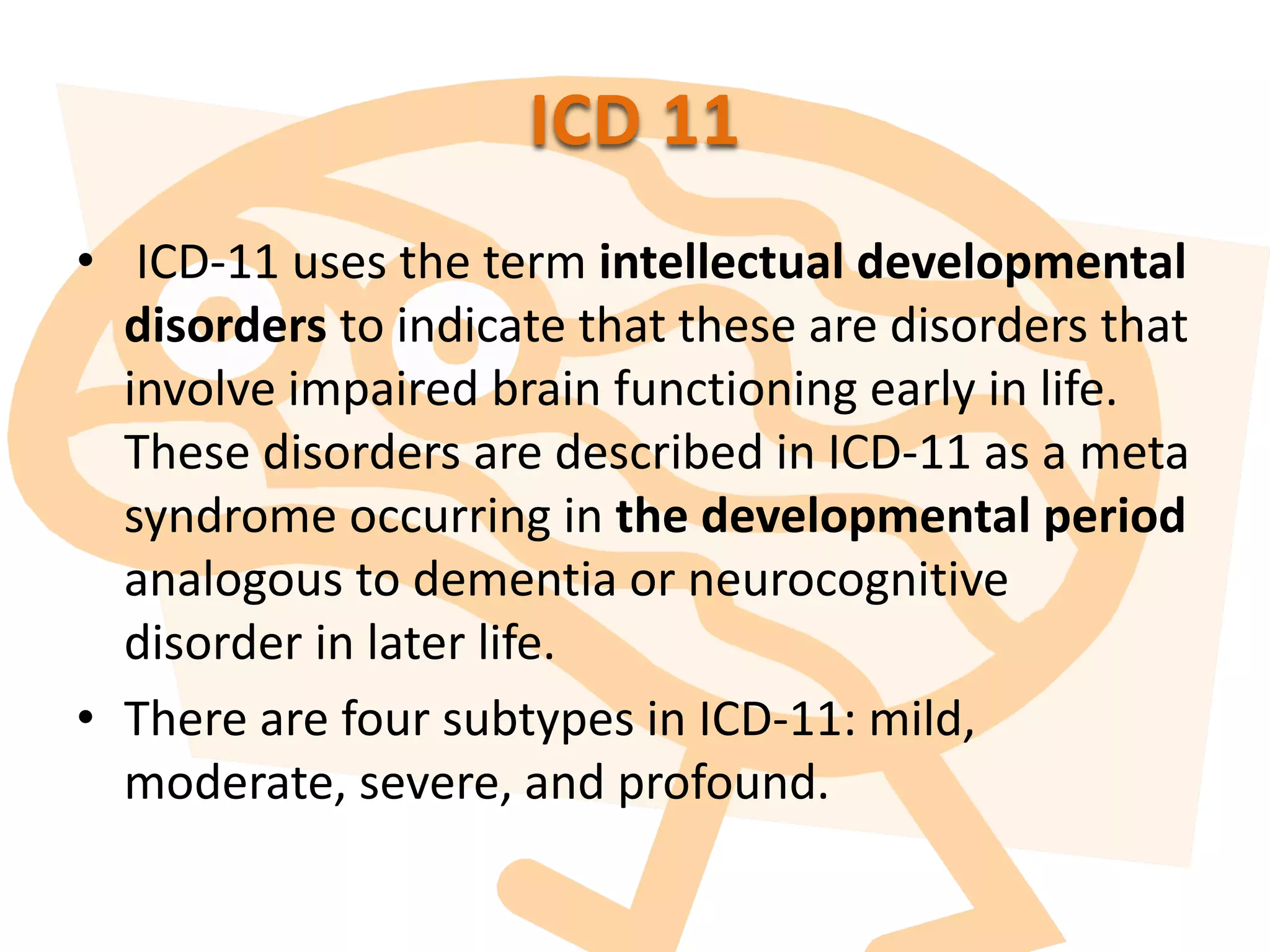











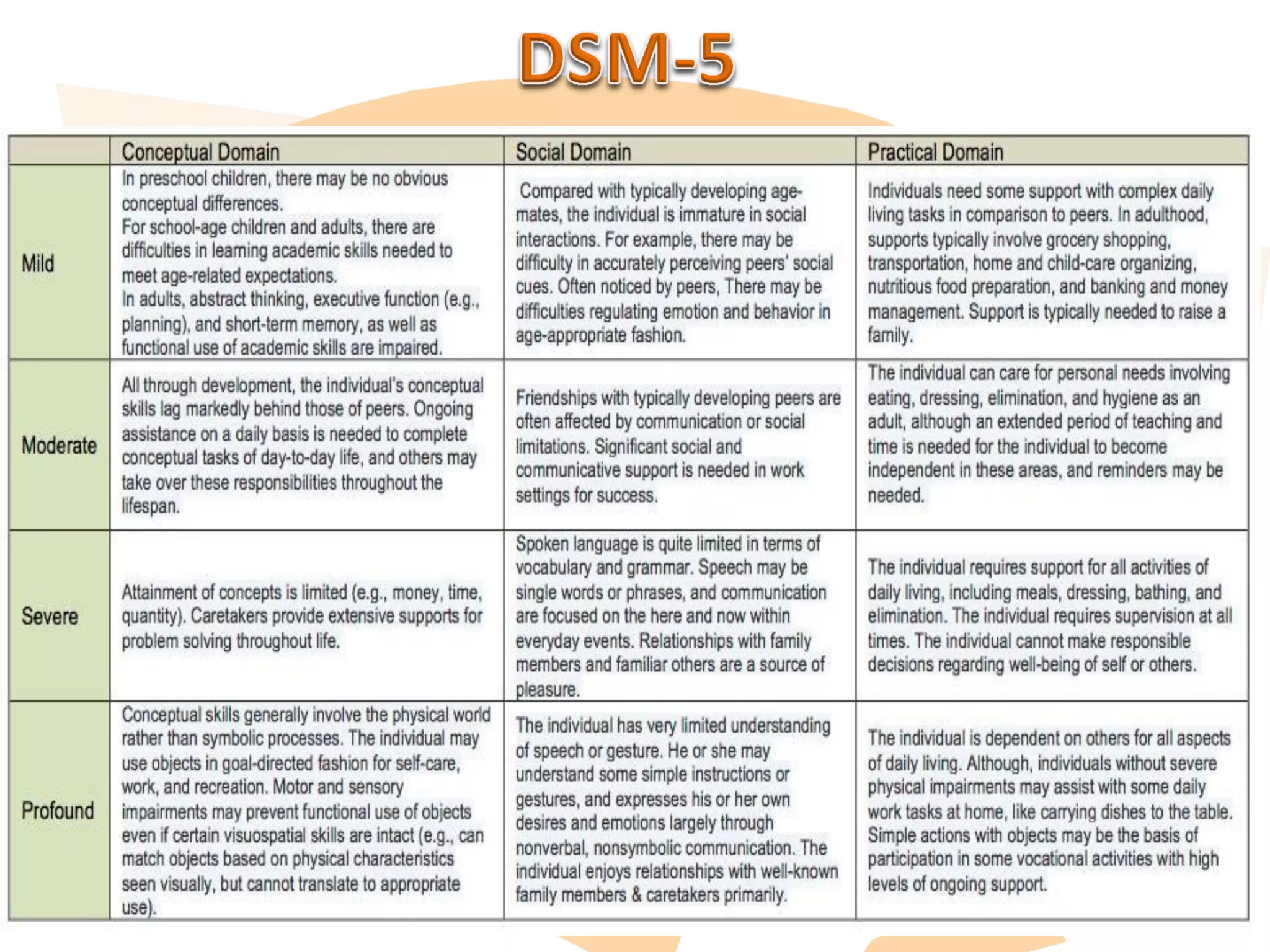







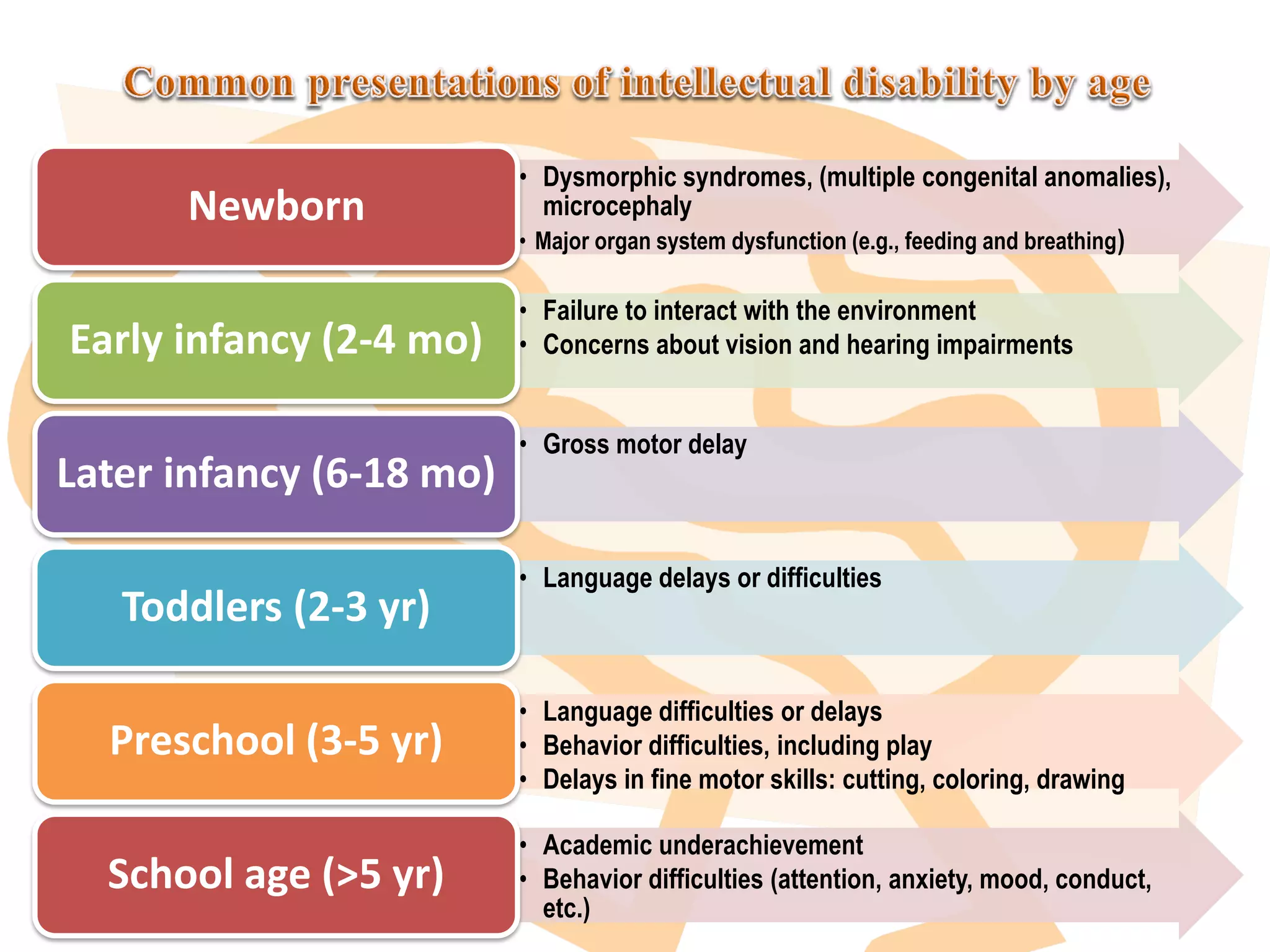
























This document discusses intellectual disability, including definitions, classifications, prevalence, causes, assessment, management, and issues faced by children with intellectual disability in the MENA region. It provides details on the DSM-5 and ICD-11 classifications and describes the assessment process. It notes that intellectual disability is often co-occurring with other neurological or mental health conditions. The document also discusses prevention, early intervention, education, and support services that can help children with intellectual disability and their families.






























![MENTAL_RETARDATION[1] by emma MAGOMA.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mentalretardation1byemmamagoma-251014190048-74e29c31-thumbnail.jpg?width=640&height=640&fit=bounds)



![Revised -ppt of child psychiatric problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pptofchildpsychiatricproblemsautosaved-240926091227-d0592556-thumbnail.jpg?width=640&height=640&fit=bounds)



















































