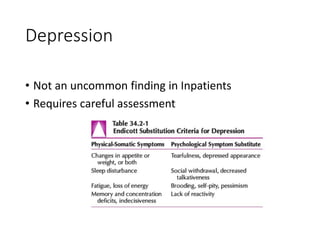
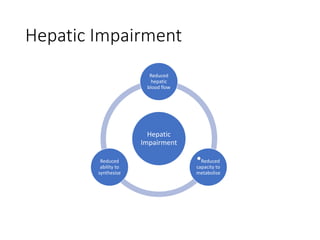
The document provides an overview of consultation-liaison psychiatry, including basics, common conditions, and management approaches. It defines consultation-liaison psychiatry and its roles in a general hospital setting. Common conditions addressed include delirium, suicide, depression, agitation, and medical issues like hepatic or renal impairment. Management prioritizes identifying and treating underlying causes, coordinating pharmacological and non-pharmacological approaches, and effective communication with medical teams.
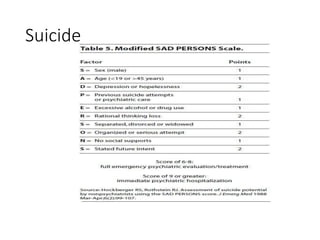





















![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)





























































