Downloaded 350 times

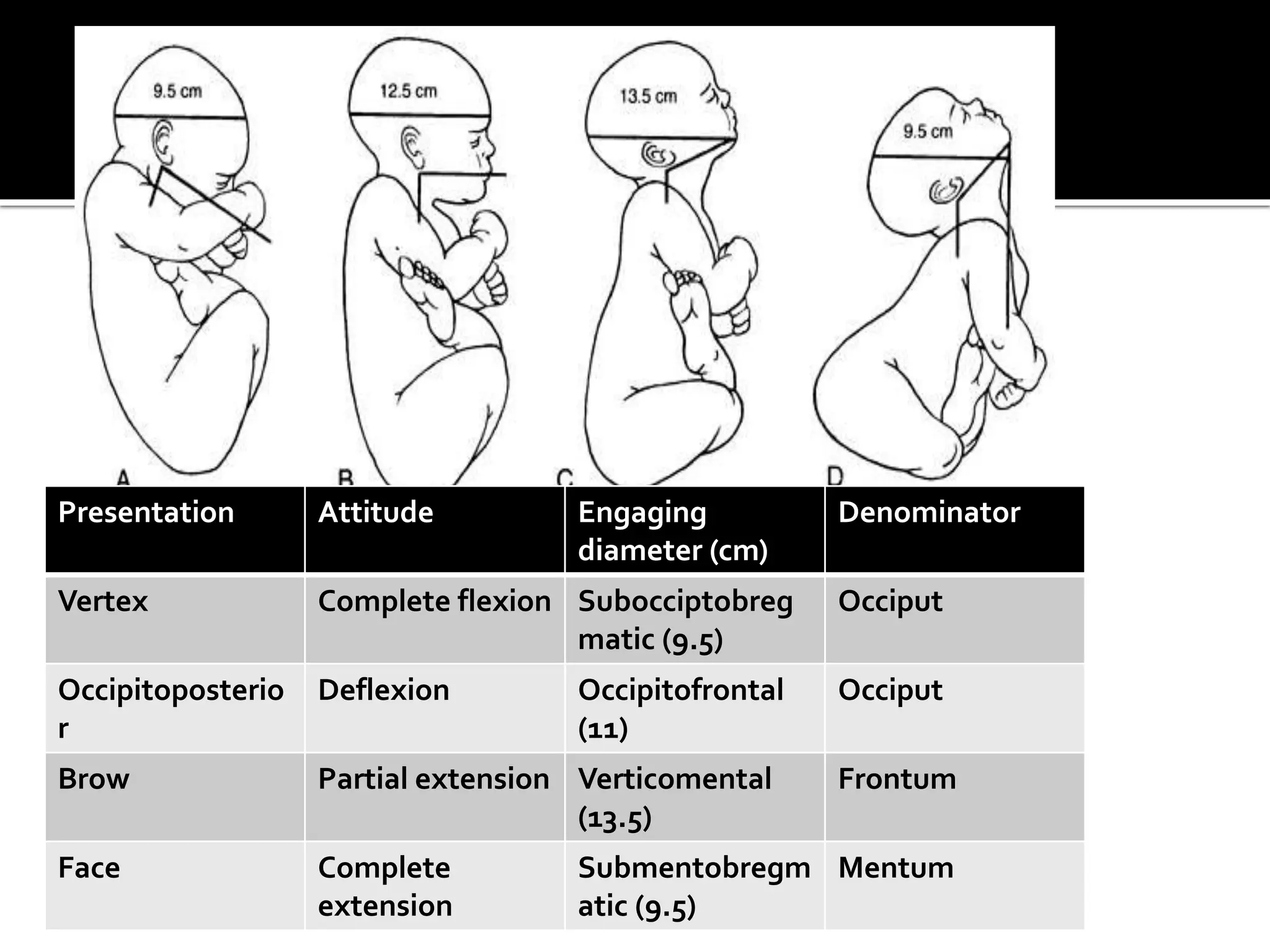
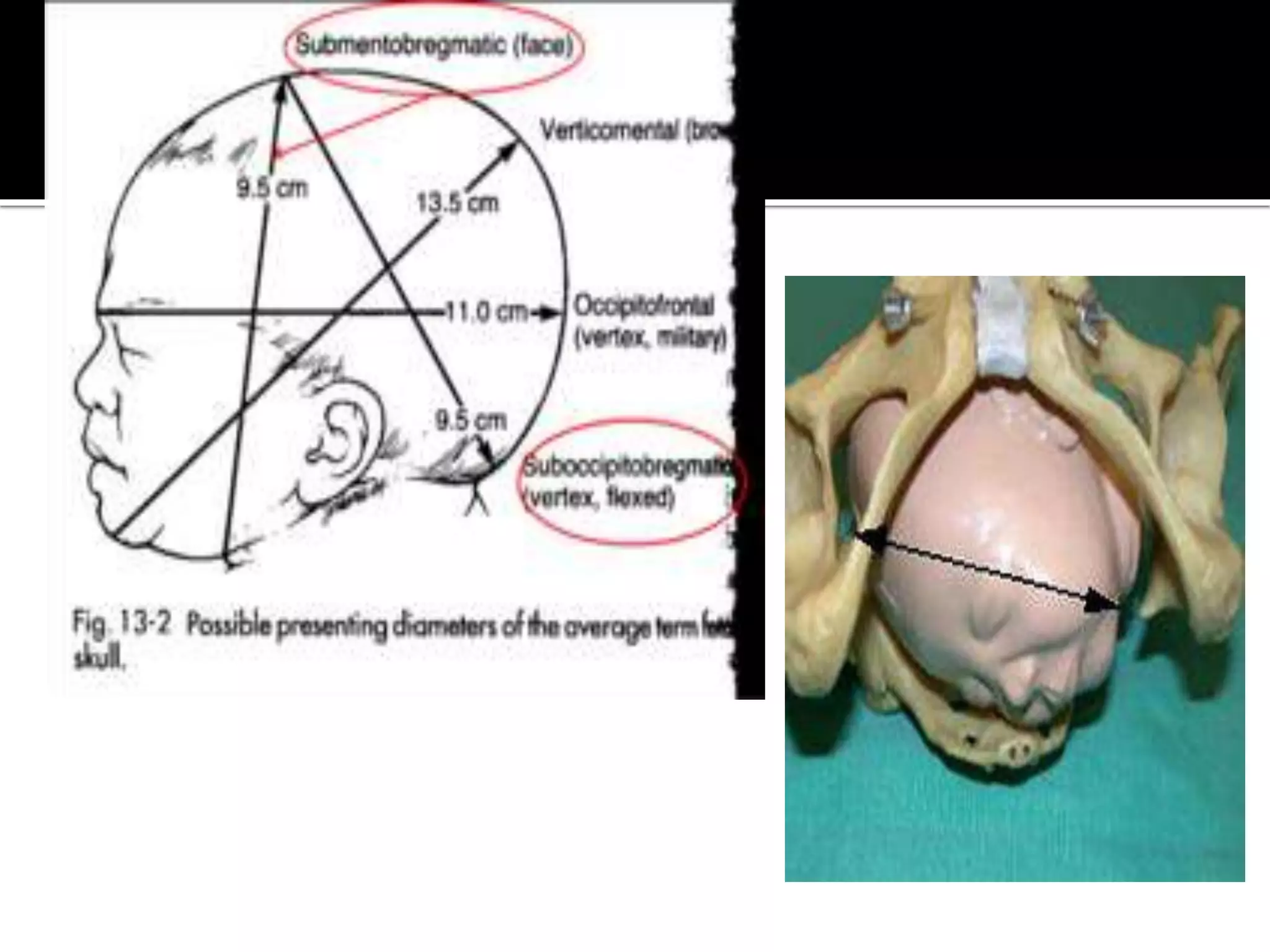
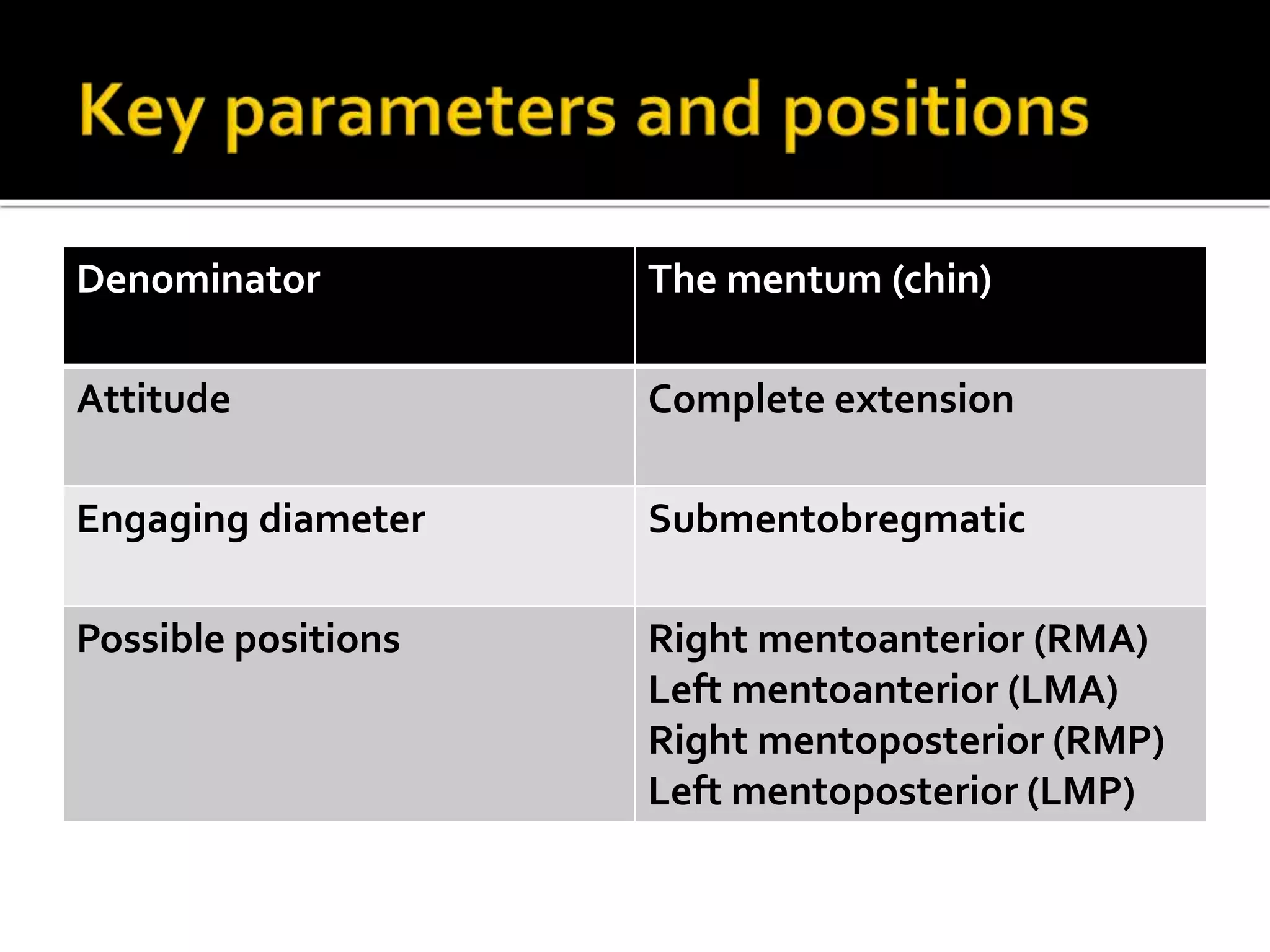
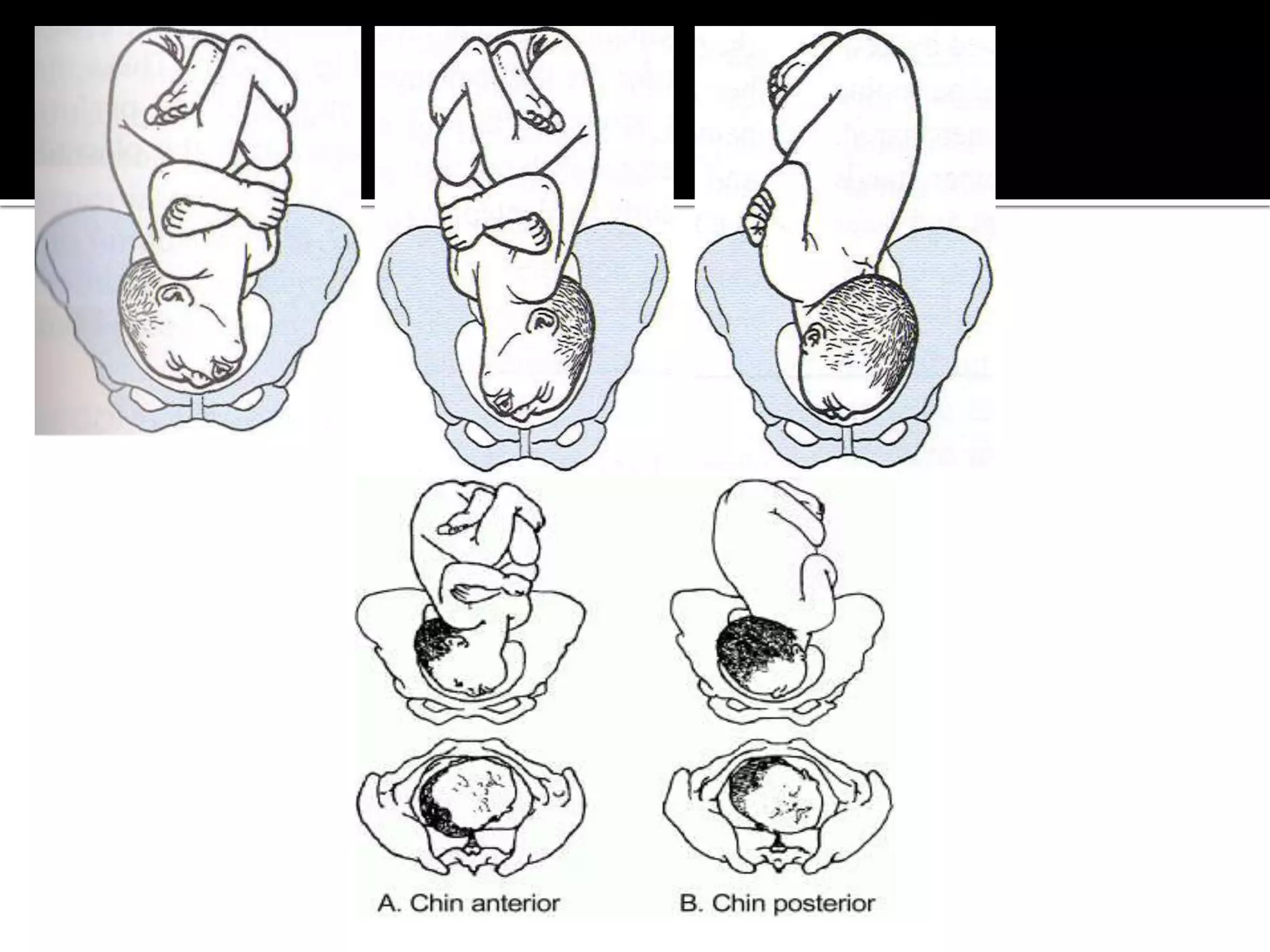
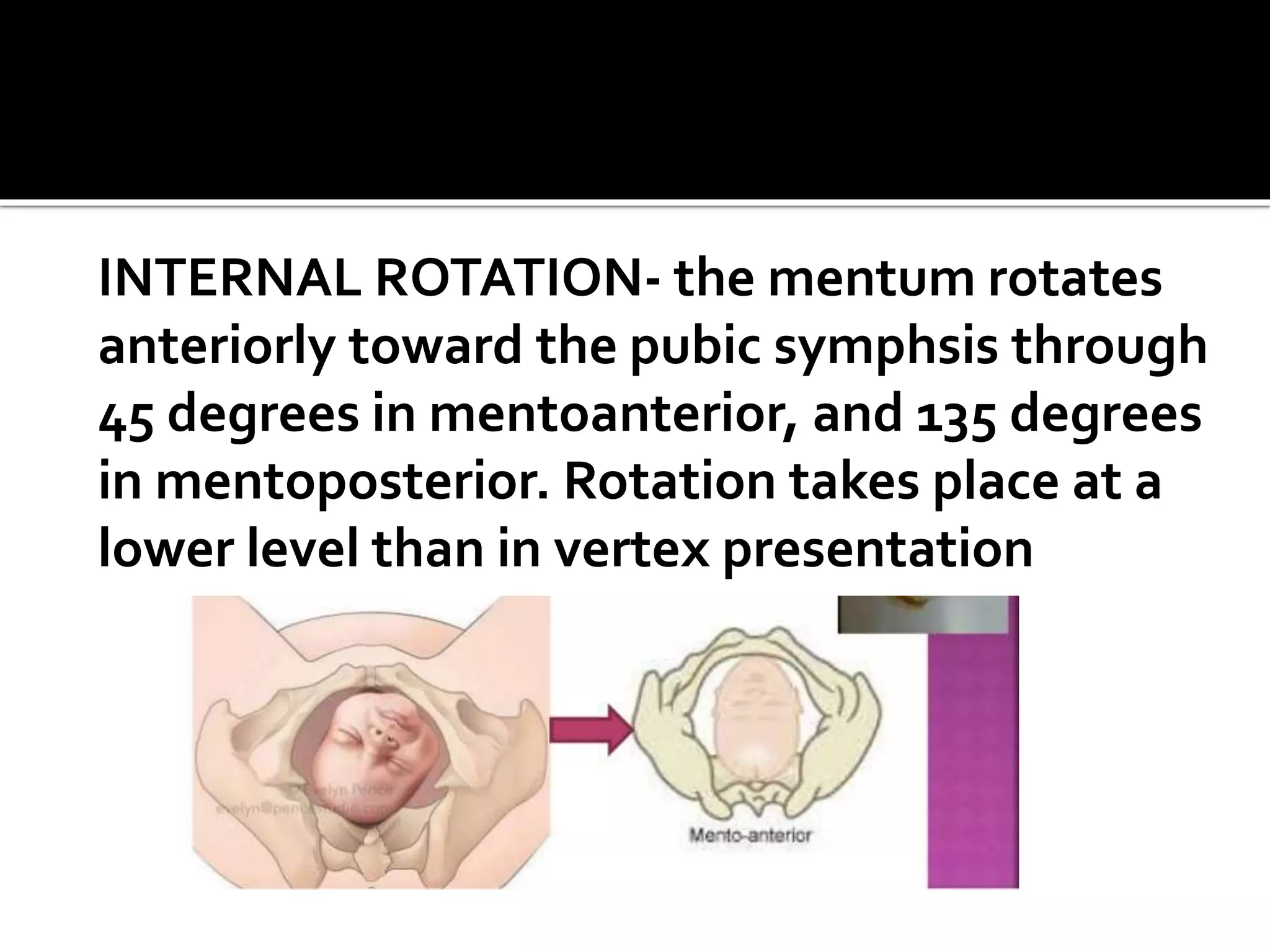
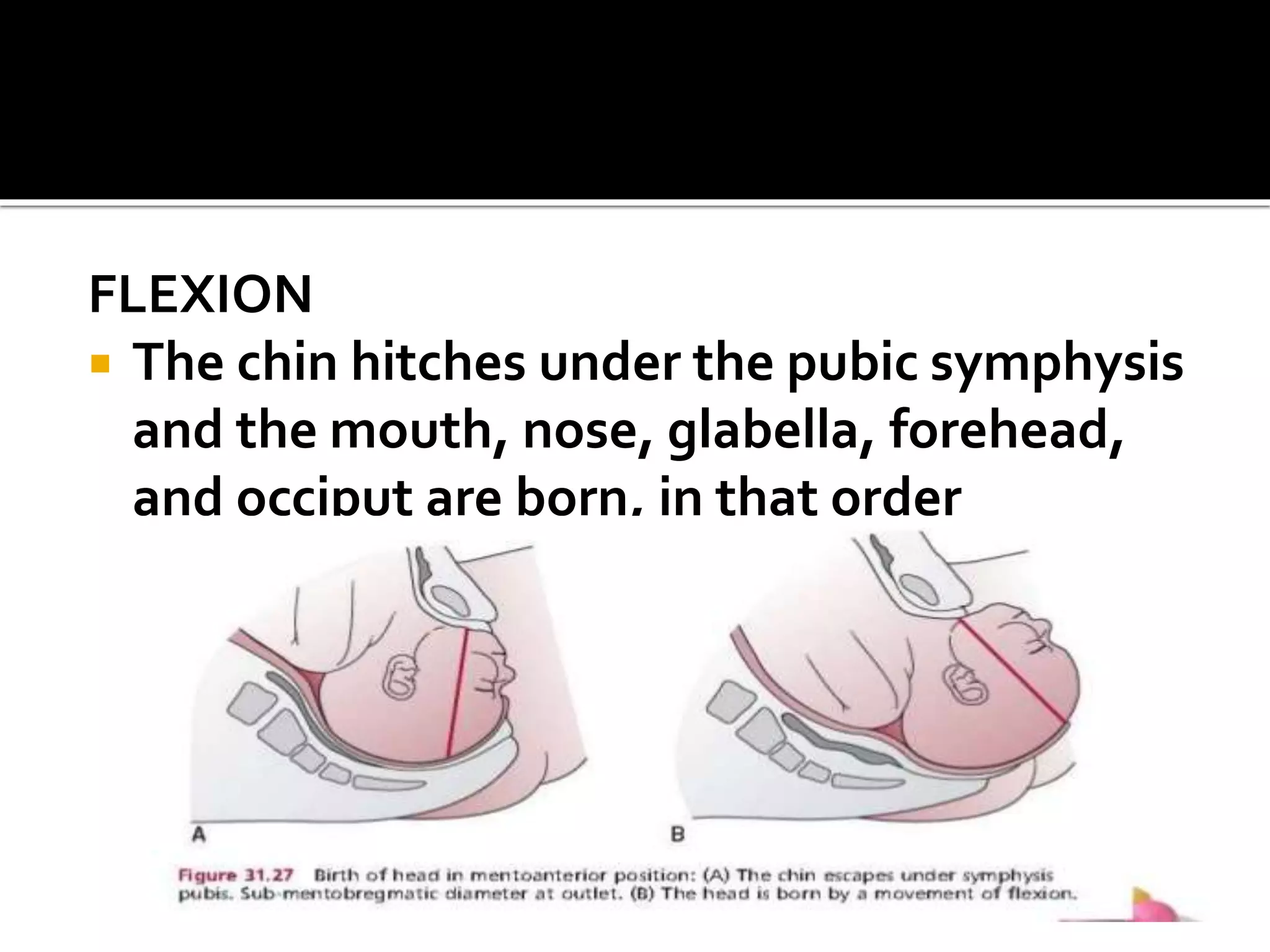
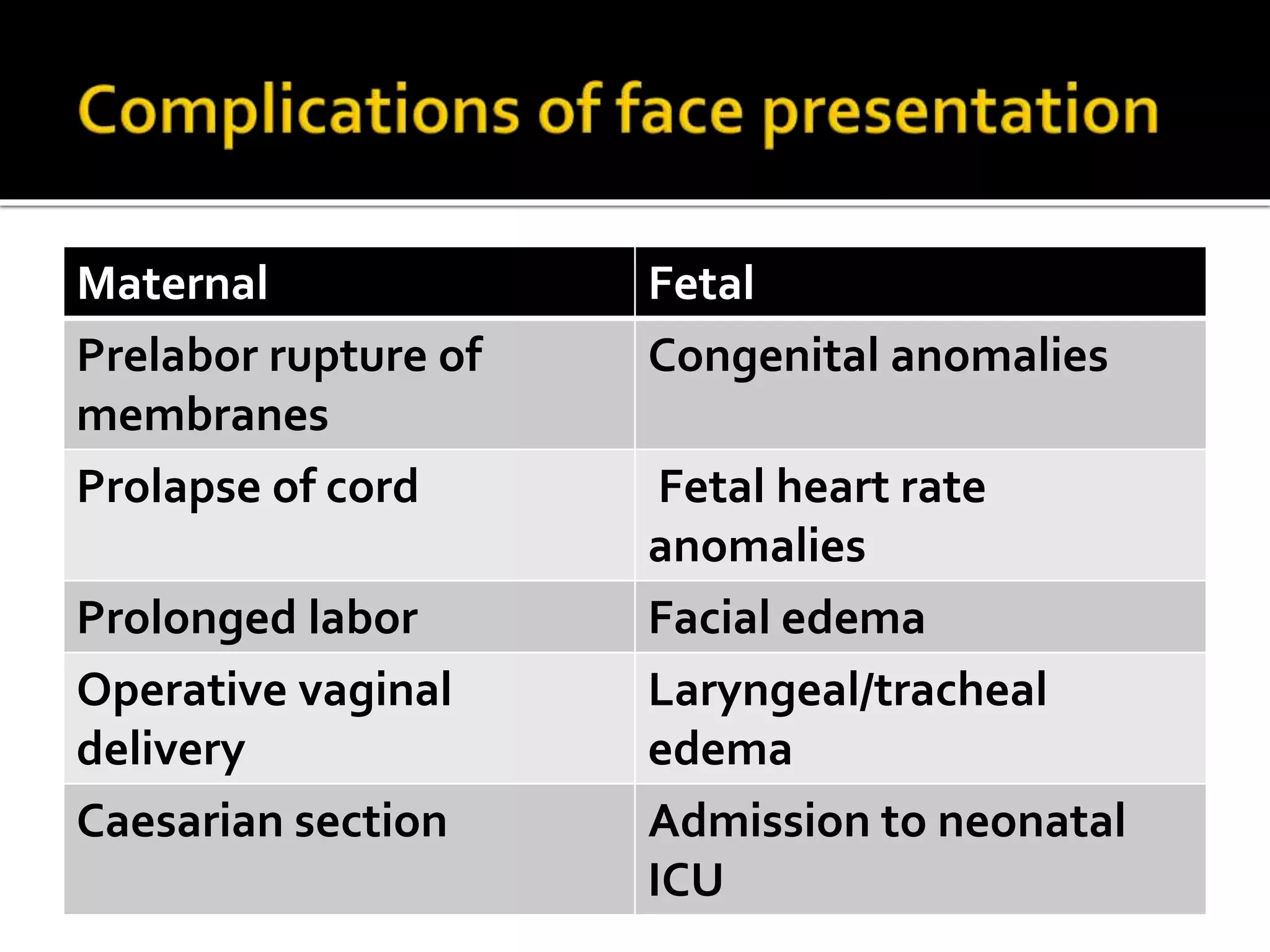
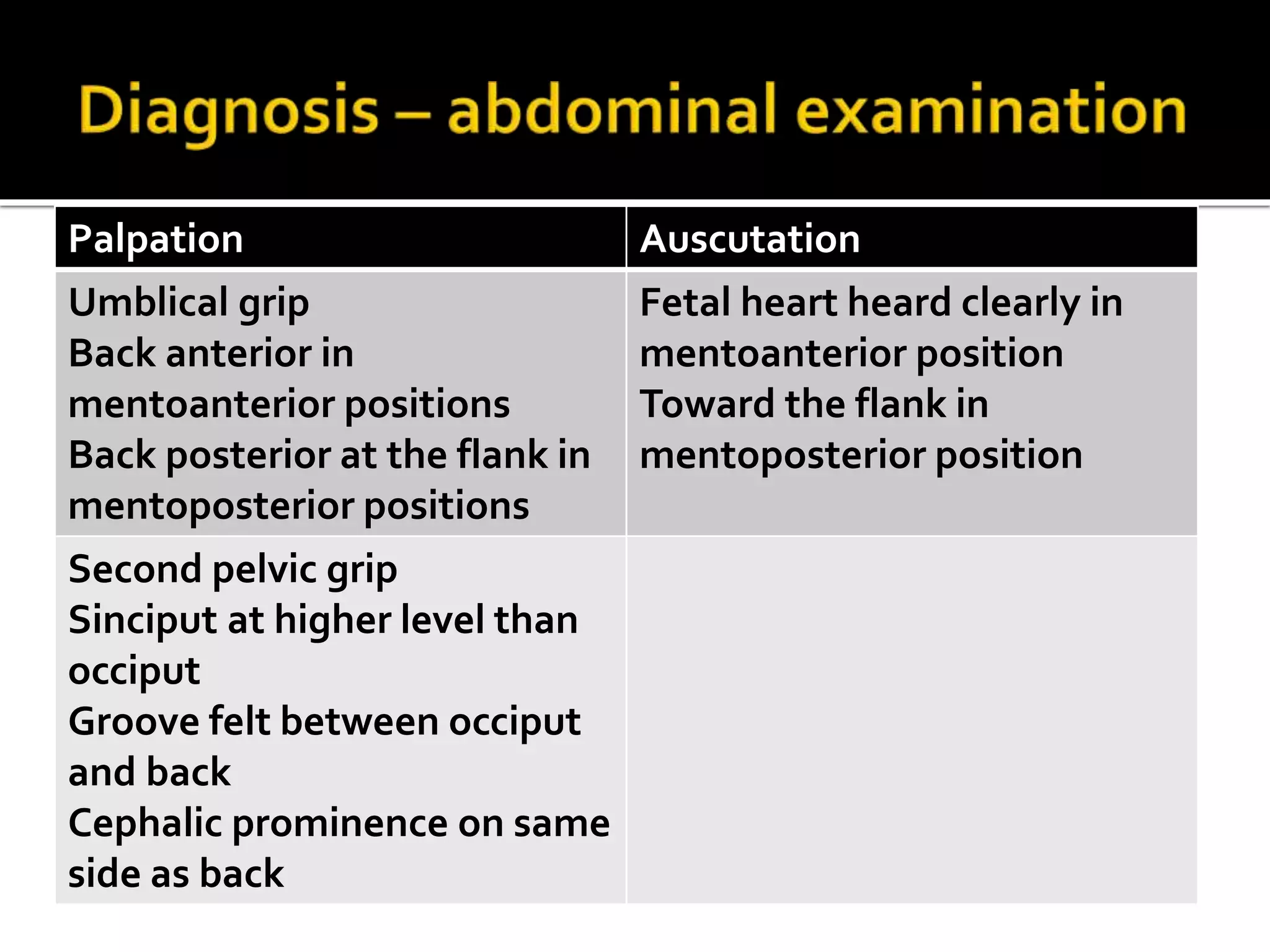
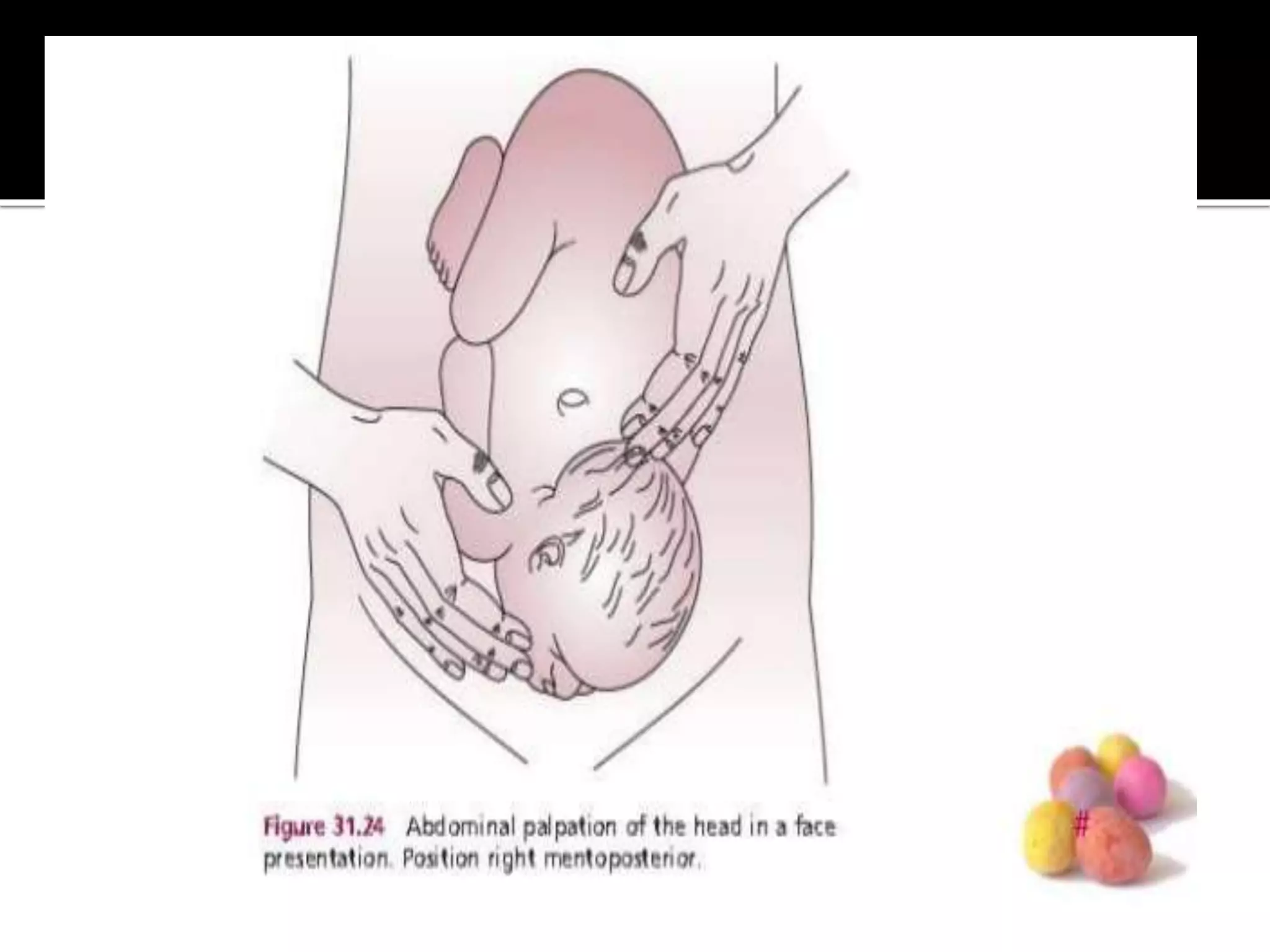
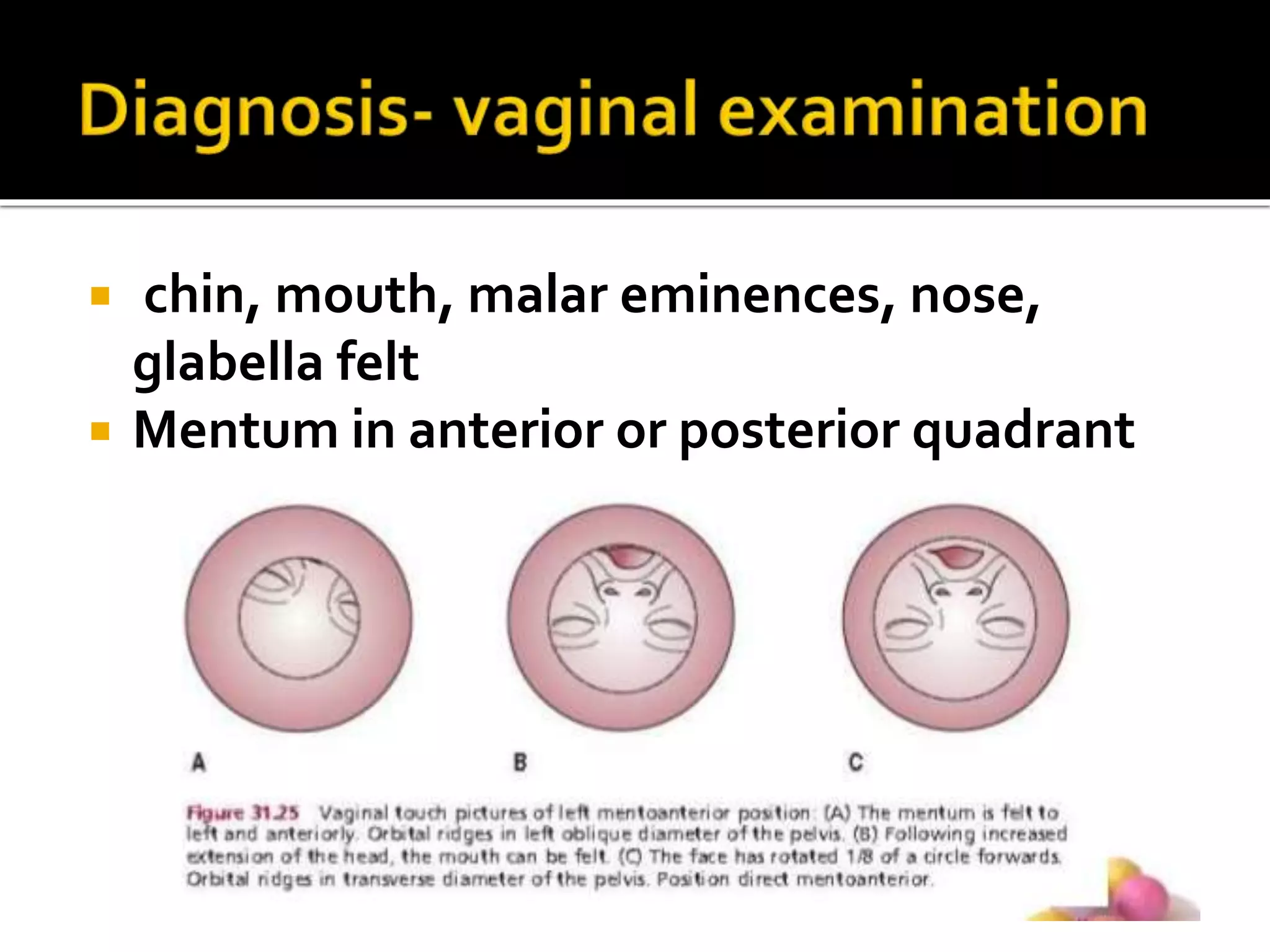
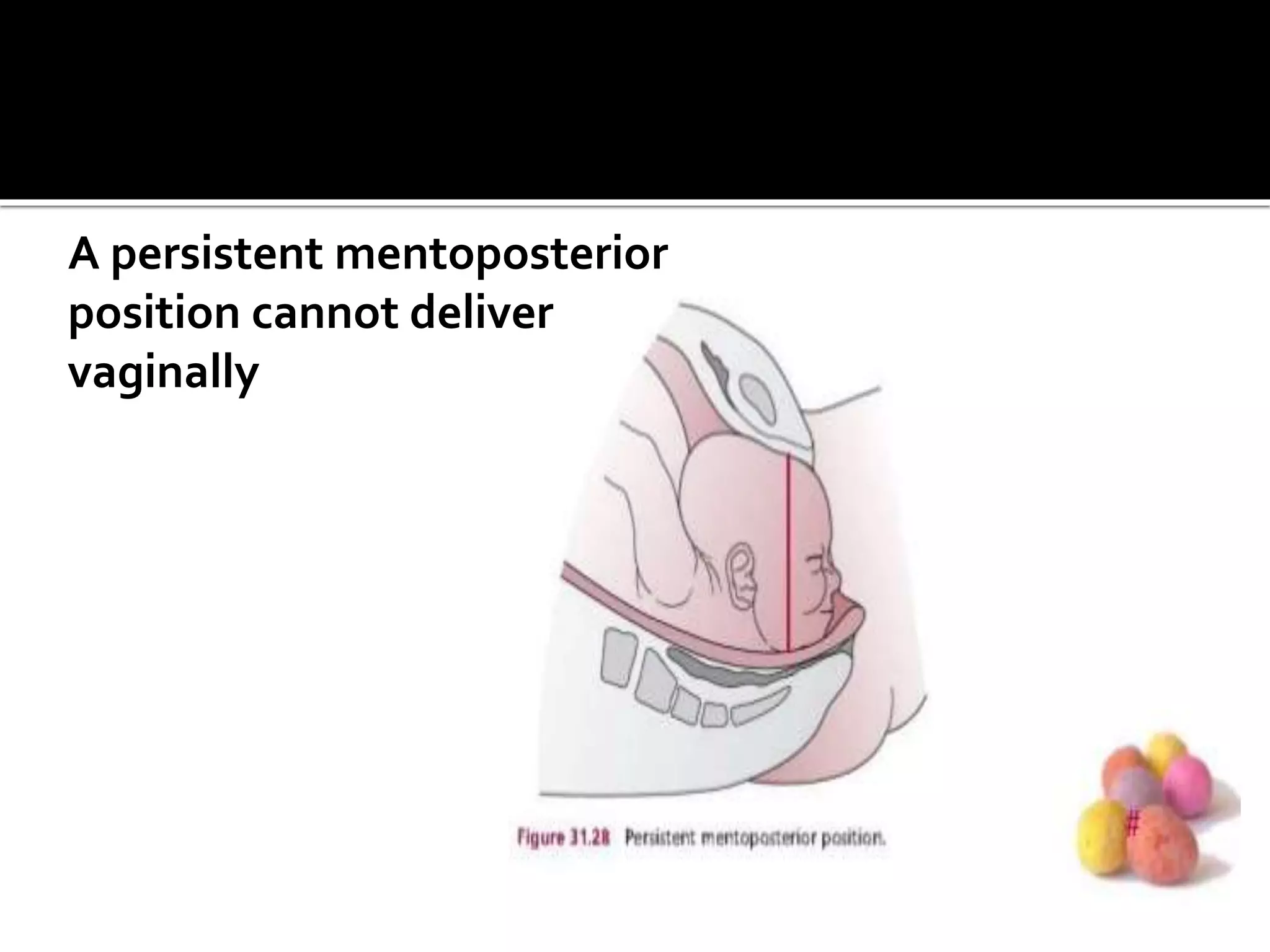
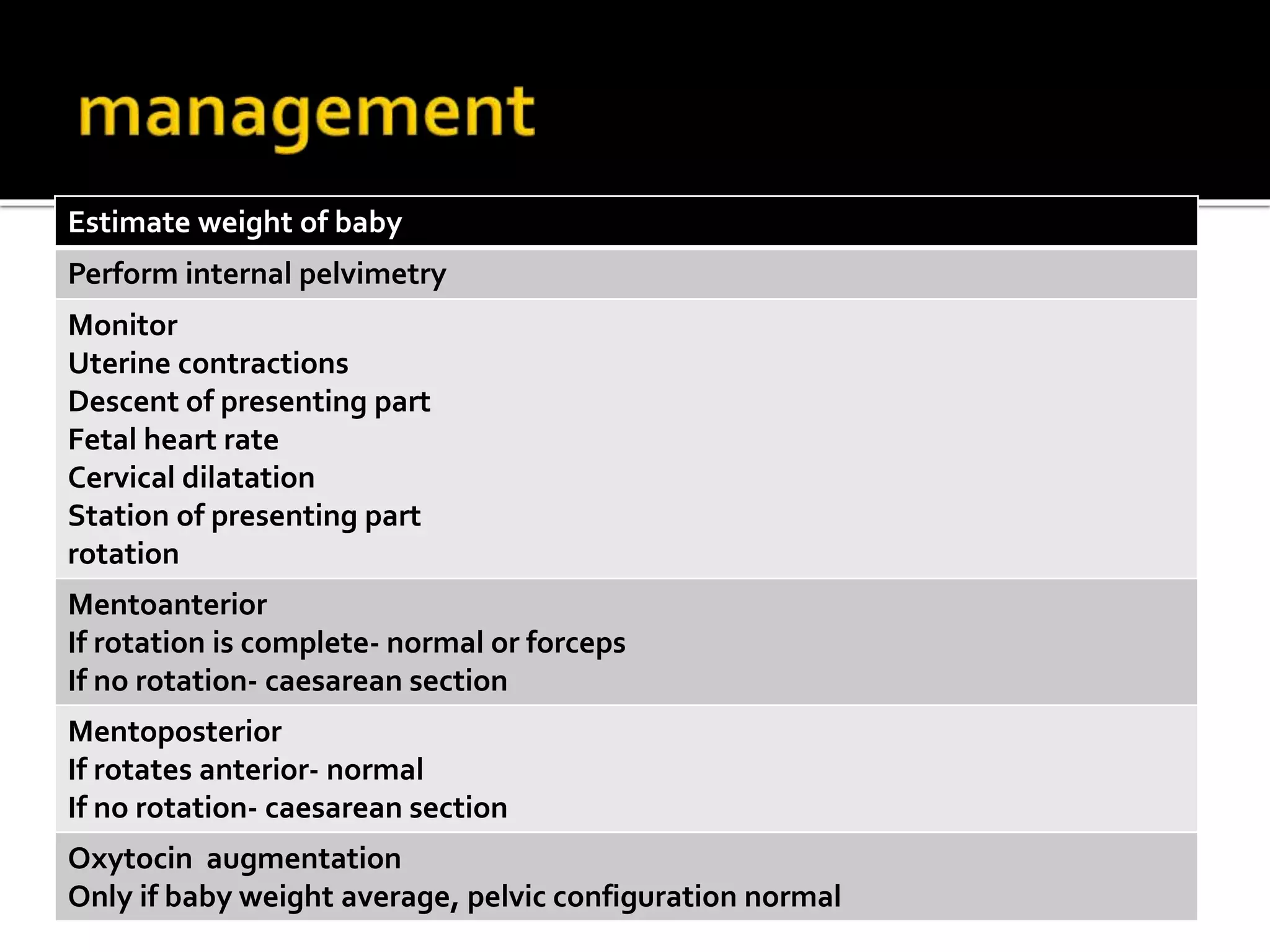
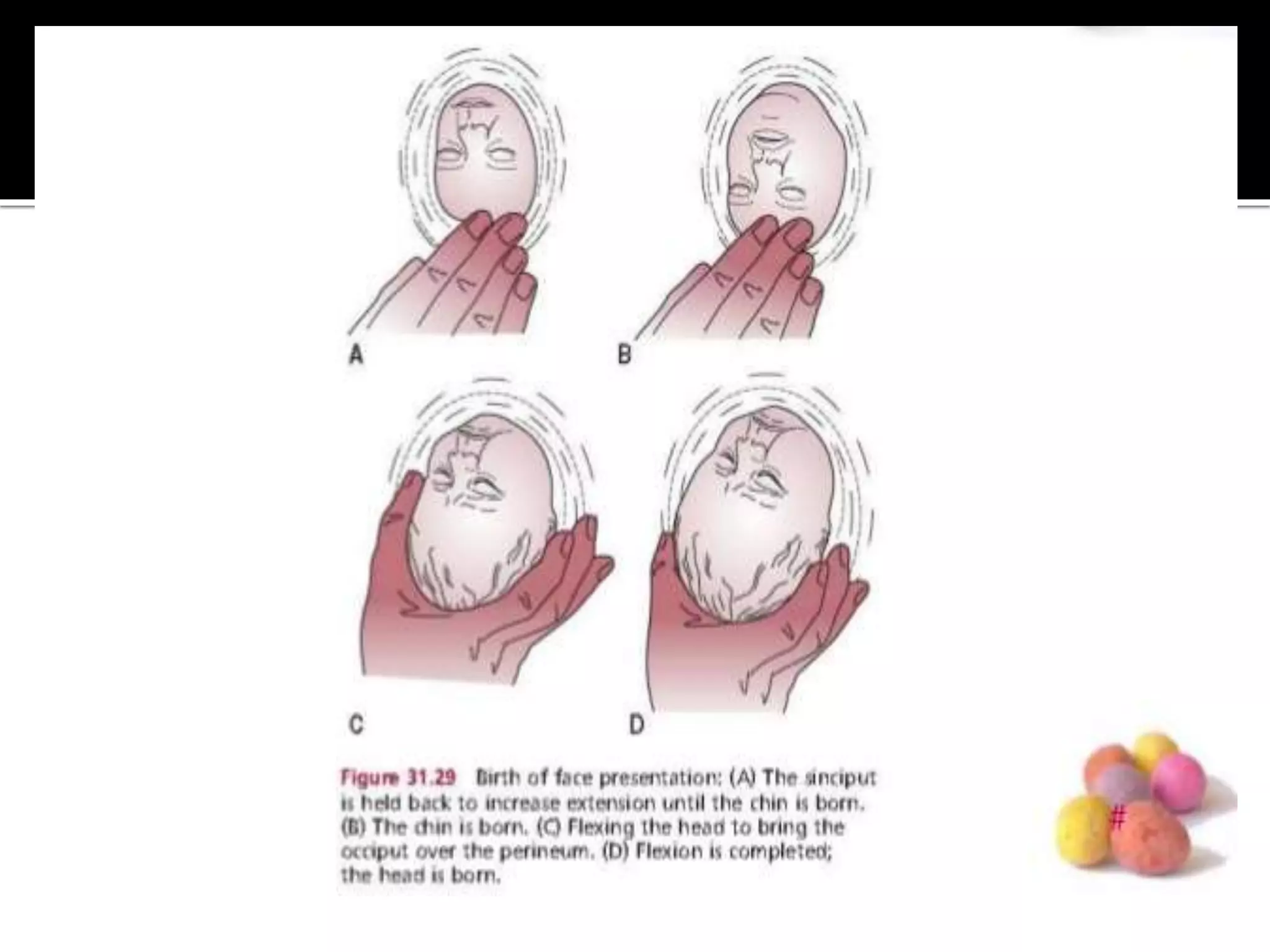
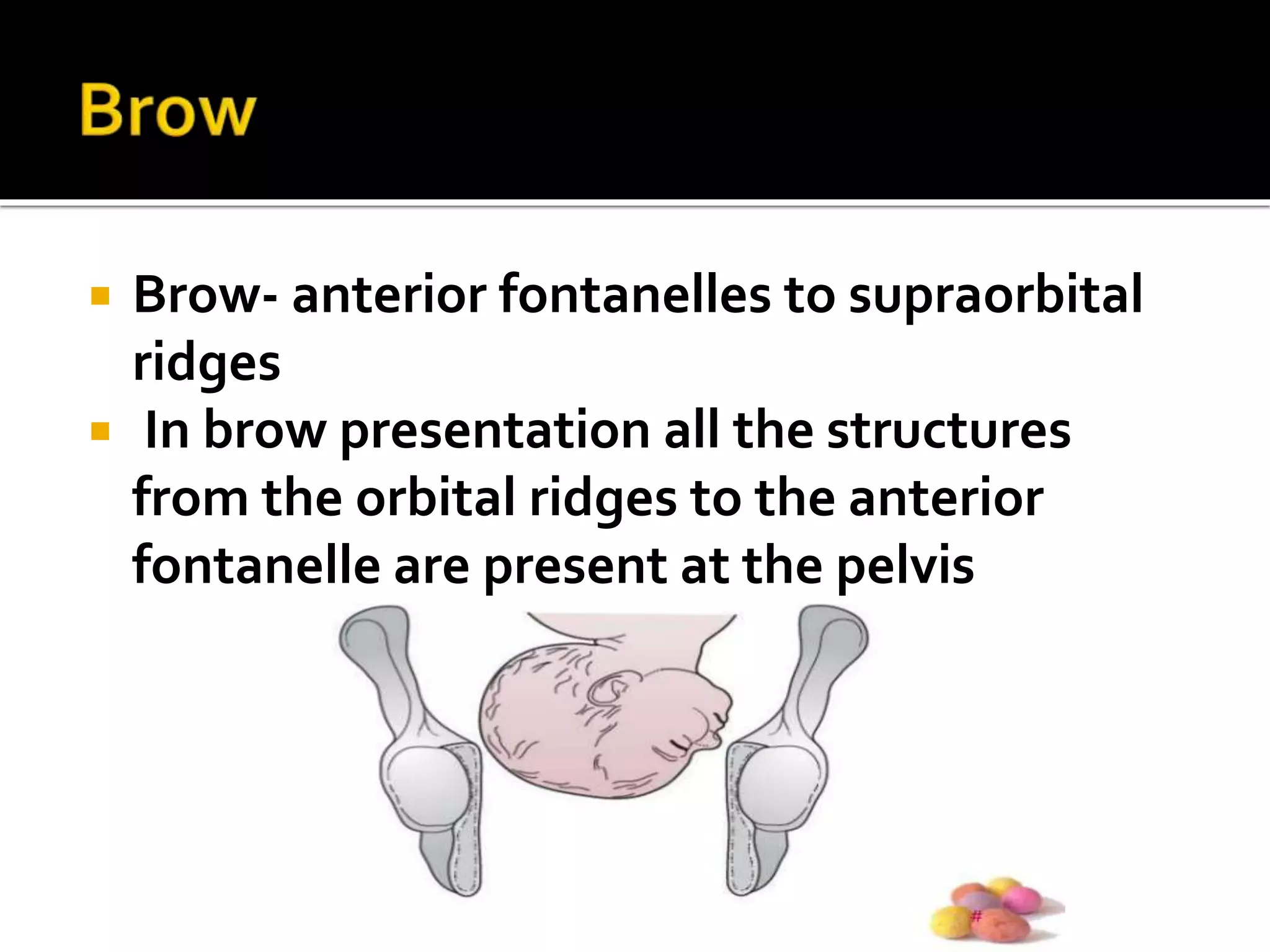

Face presentation occurs when the fetal chin presents at the pelvic inlet. The mentum engages in either a right or left oblique diameter. While mentoanterior positions often rotate anteriorly and deliver vaginally, mentoposterior positions have a 25% chance of persisting or rotating posteriorly, requiring cesarean section. Brow presentation involves the fetal forehead presenting and is not suitable for vaginal delivery due to the large engaging diameter. It usually converts to vertex or face but if persistent requires cesarean section.











































































