DEFINITION
• Abnormal descentof Umbilical cord by
side of presenting part is called
umbilical cord prolapse.
• Umbilical cord prolapse and cord
presentation are two different terms.
• Its an obstetric emergency and needs
prompt recognition and management
• Incidence 0.2-0.6% occurs 1:300
deliveries.
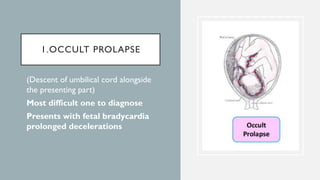
1.OCCULT PROLAPSE
• (Descentof umbilical cord alongside
the presenting part)
• Most difficult one to diagnose
• Presents with fetal bradycardia
prolonged decelerations
3.CORD PRESENTATION
Presentwith umbilical cord
between fetal presenting part and
cervix.
May occur with or without rupture
of membranes.
Pulsations of cord with Intact
membranes confirm presence of
cord presentation.
7.
OV E RA L L
I N C I D E N C E
The incidence of occult cord prolapse is unknown bcz it can be
detected only by fetal heart rate changes characteristic of
umbilical cord compression.
Overall incidence of overt cord prolapse is b/w 0.1% to 0.6%
8.
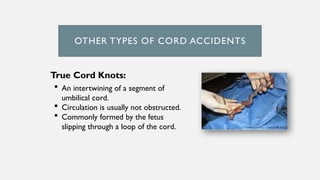
OTHER TYPES OFCORD ACCIDENTS
True Cord Knots:
An intertwining of a segment of
umbilical cord.
Circulation is usually not obstructed.
Commonly formed by the fetus
slipping through a loop of the cord.
9.
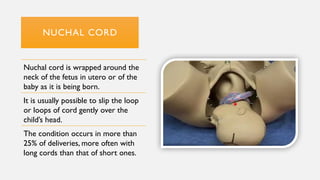
NUCHAL CORD
Nuchal cordis wrapped around the
neck of the fetus in utero or of the
baby as it is being born.
It is usually possible to slip the loop
or loops of cord gently over the
child’s head.
The condition occurs in more than
25% of deliveries, more often with
long cords than that of short ones.
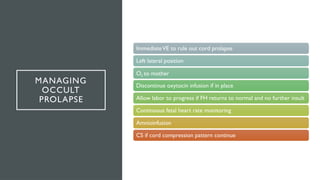
MANAGING
OCCULT
PROLAPSE
ImmediateVE to ruleout cord prolapse
Left lateral position
O2 to mother
Discontinue oxytocin infusion if in place
Allow labor to progress if FH returns to normal and no further insult
Continuous fetal heart rate monitoring
Amnioinfusion
CS if cord compression pattern continue
15.
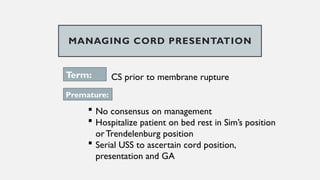
MANAGING CORD PRESENTATION
Term:CS prior to membrane rupture
Premature:
No consensus on management
Hospitalize patient on bed rest in Sim’s position
orTrendelenburg position
Serial USS to ascertain cord position,
presentation and GA
16.
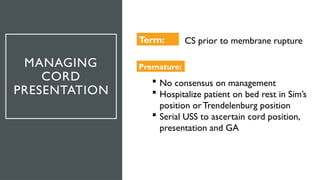
MANAGING
CORD
PRESENTATION
Term: CS priorto membrane rupture
Premature:
No consensus on management
Hospitalize patient on bed rest in Sim’s
position orTrendelenburg position
Serial USS to ascertain cord position,
presentation and GA
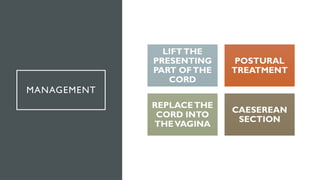
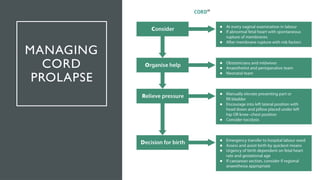
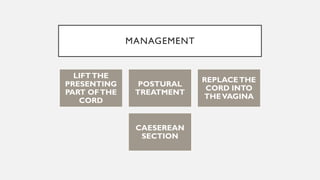
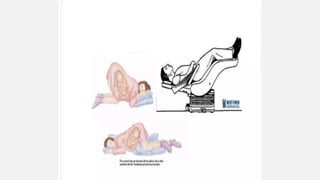
MANAGING
CORD PROLAPSE
Speed isof the essence and perinatal outcome is
largely dictated by diagnosis delivery interval.
Three components of management are:
1.Prevent or relieve cord compression and vasospasm
2.Fetal assessment
3.Prompt delivery of the infant
Speed is ofthe essence and perinatal outcome is largely dictated by
diagnosis delivery interval.
Three components of management are:
2.Fetal assessment
3.Prompt delivery of the infant
1.Prevent or relieve cord compression and vasospasm
28.
PREVENTION
Women with transverse,oblique or
unstable lie should be offered elective
admission to hospital at 37 weeks of
gestation, or sooner if there are signs
of labour or suspicion
Women with non-cephalic
presentations and preterm pre-labour
rupture of the membranes should be
offered admission
29.
PREVENTION
• Women withtransverse, oblique or unstable lie
should be offered elective admission to hospital at
37 weeks of gestation, or sooner if there are signs of
labour or suspicion
• Women with non-cephalic presentations and
preterm pre-labour rupture of the membranes
should be offered admission
30.
PREVENTION
Women with transverse,oblique or
unstable lie should be offered elective
admission to hospital at 37 weeks of
gestation, or sooner if there are signs
of labour or suspicion
Women with non-cephalic
presentations and preterm pre-labour
rupture of the membranes should be
offered admission