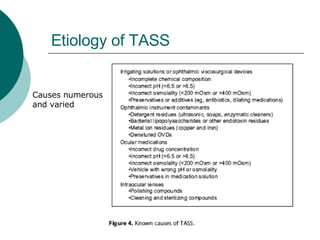
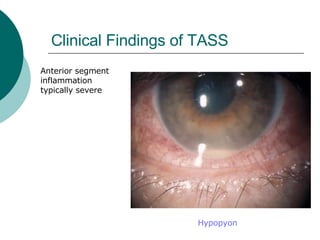
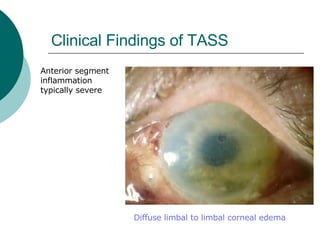
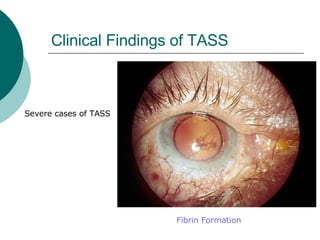
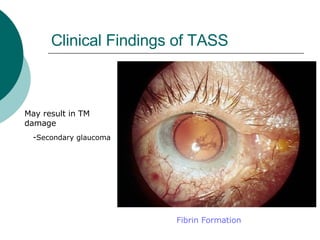
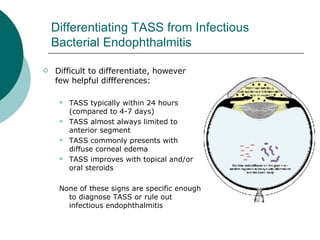
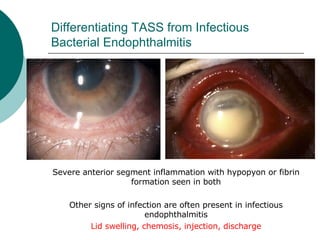
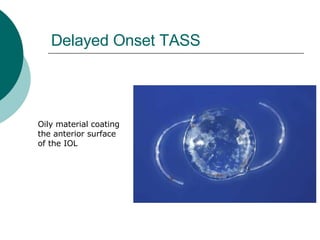
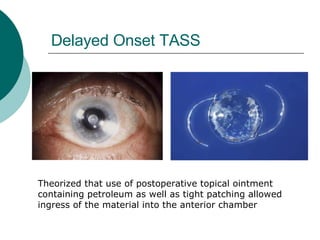
This document summarizes a journal article on toxic anterior segment syndrome (TASS). TASS is a non-infectious inflammatory reaction caused by a toxic substance entering the anterior segment during eye surgery. Common causes include preservatives inadvertently injected into the eye, detergents or residues left on instruments, and contaminated water or solutions. TASS presents with pain, blurred vision, eye redness, and severe anterior segment inflammation including corneal edema and hypopyon. Treatment involves topical steroids, but prevention through proper sterilization and use of preservative-free solutions is key to avoiding this complication.