Downloaded 102 times
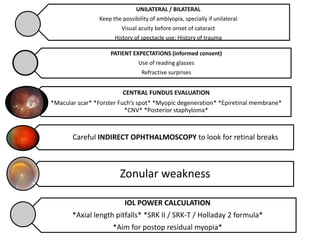
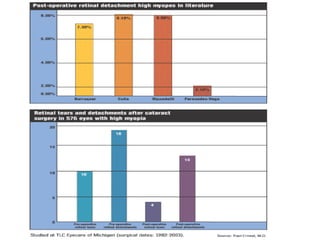
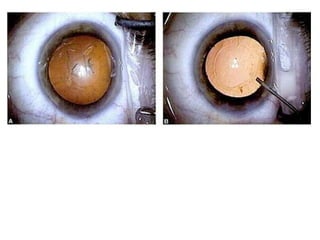
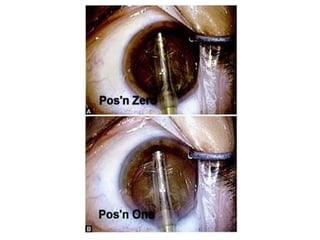


This document discusses considerations for phacoemulsification cataract surgery in myopic eyes. Key points addressed include: - Myopic eyes have a thinner sclera and weaker zonules, requiring special care during surgery like using clear corneal incisions and suturing if needed. - The anterior chamber is deeper in myopic eyes, making instrumentation more difficult and increasing risks like iris stretching and reverse pupillary block. - Careful preoperative evaluation of the fundus is important to assess for macular pathology, retinal breaks, or high myopia that could impact outcomes. - Intraocular lens power calculation and choice is more complex in myopic eyes to aim for residual myopia and account for axial length



































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

