
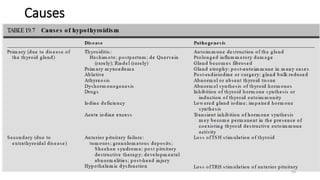

The document discusses thyroid gland disorders and hypothyroidism. It provides details on the causes, effects on organ systems, and types of hypothyroidism. The main causes of hypothyroidism are autoimmune thyroiditis, which results in the gradual destruction of the thyroid gland, and surgical or medical thyroid ablation for conditions like Graves' disease. Hypothyroidism can affect many organ systems by reducing the basal metabolic rate and impairing other metabolic processes. It discusses the different types of hypothyroidism, including congenital hypothyroidism and central hypothyroidism.
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






