Downloaded 152 times
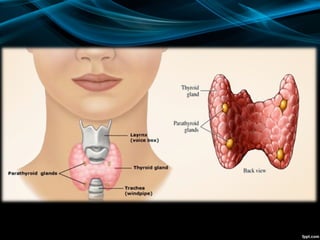
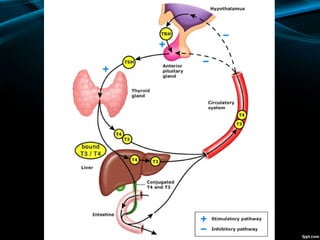









The document discusses the physiology of the thyroid gland and thyroid hormones such as T3 and T4. It describes how the pituitary-thyroid axis controls thyroid hormone production and discusses different types of thyroid enlargement including simple goiter, diffuse hyperplastic goiter, toxic nodular goiter, and Graves' disease. The principles and advantages/disadvantages of different treatment approaches for hyperthyroidism are provided, including anti-thyroid drugs, surgery, and radioiodine therapy. Potential postoperative complications of thyroid surgery are also listed.






























![THYROID_GLAND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidgland1-231005071359-bdb08841-thumbnail.jpg?width=640&height=640&fit=bounds)






















![lec 14 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lec14autosaved-230315142106-831cdef1-thumbnail.jpg?width=640&height=640&fit=bounds)