Introduction
☛Bethesda System forReporting
Thyroid Cytopathology (BSRTC)
recommends that each thyroid FNA
report should begin with a general
diagnostic category.
☛The motive behind is to bring clarity
of communication amongst
pathologists and amongst
pathologist and clinicians.
3.
1. Nondiagnostic orUnsatisfactory
2. Benign
3. Atypia of Undetermined Significance or
Follicular Lesion of Undetermined
Significance
4. Follicular Neoplasm or Suspicious for a
Follicular Neoplasm
5. Suspicious for Malignancy
6. Malignant
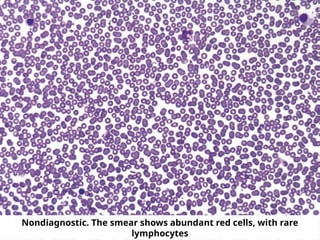
☛Fewer than sixgroups of well-
preserved, well-stained follicular cell
groups with ten cells each
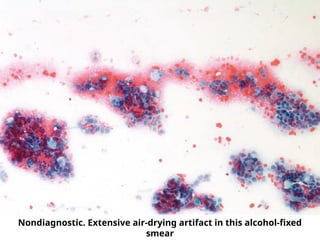
☛Poorly prepared, poorly stained, or
obscured follicular cells
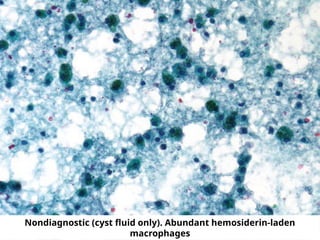
☛Cyst fluid, with or without histiocytes,
and fewer than six groups of ten
benign follicular cells
Exceptions
1. Solid noduleswith cytologic atypia
• Any significant atypia has to be reported
• Minimum number of cells not required
2. Solid nodules with inflammation
• Thyroiditis may show only infammatory
cells
• Minimum number of cells not required
3. Colloid nodules
• Minimum number of cells is not
required if easily-identifiable colloid
Benign Follicular Nodules(BFNs)
● nodules in nodular goiter (NG)
● hyperplastic (adenomatoid) nodules
● colloid nodules
● nodules in Graves’ disease
● subset of follicular adenomas (those of
macrofollicular type)
Thyroiditis
● Lymphocytic, Acute, Sub-acute, Riedel’s
12.
Benign Follicular Nodule
☛Colloid
● dark blue-violet-magenta with
Romanowsky
● green to orange-pink with
Papanicolaou
● Thin colloid - “thin membrane/cellophane”
or “crazy pavement” or “chicken wire”
or mosaic appearance
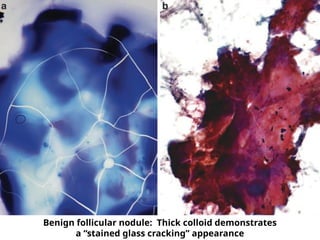
● Dense colloid - hyaline quality and shows
cracks
☛ Follicular cells - arranged predominantly in
monolayered sheets and are evenly spaced
13.
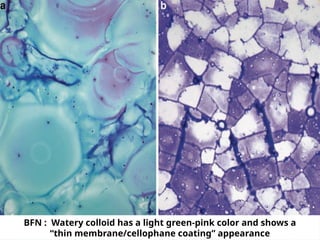
BFN : Waterycolloid has a light green-pink color and shows a
“thin membrane/cellophane coating” appearance
BFN : Predominantlymonolayered sheets of follicular cells are
admixed with occasional pigment-laden macrophages
16.
Grave’s Disease
☛ Lymphocytesmay be seen in the
background.
☛ Follicular cells are arranged in flat sheets
and loosely cohesive groups, with
abundant delicate, foamy cytoplasm.
☛ Nuclei are often enlarged, vesicular, and
show prominent nucleoli.
☛ Few microfollicles may be observed.
☛ Distinctive flame cells may be prominent,
and are represented by marginal
cytoplasmic vacuoles with red to pink
17.
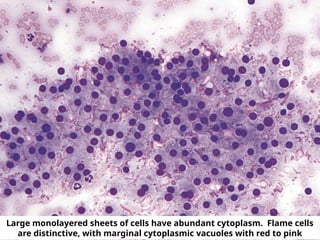
Large monolayered sheetsof cells have abundant cytoplasm. Flame cells
are distinctive, with marginal cytoplasmic vacuoles with red to pink
18.
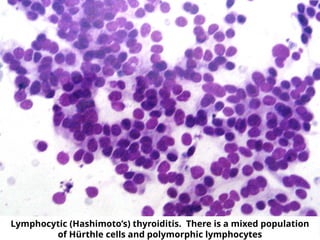
Hashimoto’s Thyroiditis
☛ Usuallyhypercellular, but does not require
a minimum number of follicular/Hürthle
cells for adequacy.
☛ The lymphoid population is polymorphic,
including small mature lymphocytes,
larger reactive lymphoid cells, and
occasional plasma cells.
☛ Hürthle cells (oncocytes), when present,
are arranged in sheets or as isolated cells.
They have abundant granular cytoplasm,
large nuclei, and prominent nucleoli
Granulomatous/de Quervain’s
thyroiditis
☛ Clustersof epithelioid histiocytes, i.e.,
granulomas, are present along with many
multinucleated giant cells.
☛ Early stage - many neutrophils and
eosinophils, similar to acute thyroiditis.
☛ Late stages - smears are hypocellular. They
show giant cells surrounding and
engulfing colloid, epithelioid cells,
lymphocytes, macrophages, and scant
degenerated follicular cells
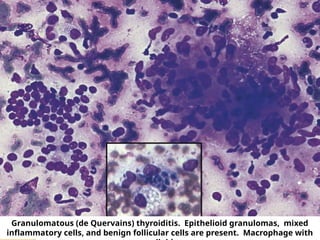
21.
Granulomatous (de Quervains)thyroiditis. Epithelioid granulomas, mixed
inflammatory cells, and benign follicular cells are present. Macrophage with
22.
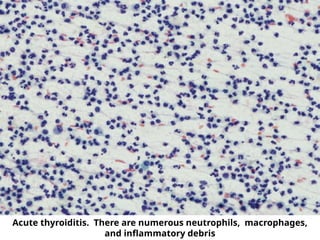
Acute thyroiditis
☛ Numerousneutrophils are associated with
necrosis, fibrin, macrophages and blood.
☛ There are scant reactive follicular cells and
limited to absent colloid.
☛ Bacterial or fungal organisms are
occasionally seen in the background
especially in immunocompromised
patients.
Riedel’s Thyroiditis
☛The thyroidgland feels stony hard on
palpation.
☛The preparations are often acellular.
☛Collagen strands and bland spindle cells
may be present.
☛There are rare chronic inflammatory
cells.
☛Colloid and follicular cells are usually
absent
25.
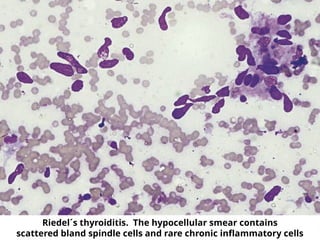
Riedel´s thyroiditis. Thehypocellular smear contains
scattered bland spindle cells and rare chronic inflammatory cells
26.
Category III
Atypia ofUndetermined
Significance/Follicular
Lesion of Undetermined
Significance
27.
☛ specimens thatcontain cells
(follicular, lymphoid, or other) with
architectural and/or nuclear atypia
that is not sufficient to be classified
as suspicious for a follicular
neoplasm, suspicious for malignancy
or malignant
☛ On the other hand, the atypia is
more marked than can be ascribed
confidently to benign changes
28.
Examples :
☛ Predominanceof Hürthle cells in a sparsely
cellular aspirate with scant colloid
☛Focal features suggestive of papillary
carcinoma in an otherwise predominantly
benign-appearing sample
☛Cyst-lining cells which may appear atypical
due to nuclear features in an otherwise
predominantly benign-appearing sample.
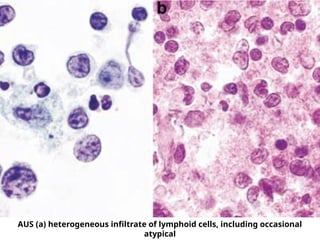
☛Atypical lymphoid infiltrate but the degree
of atypia is insufficient for the general
category “suspicious for malignancy.”
29.
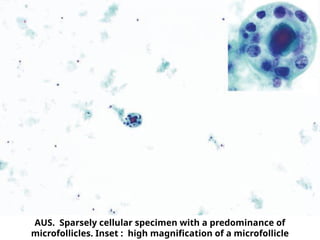
AUS. Sparsely cellularspecimen with a predominance of
microfollicles. Inset : high magnification of a microfollicle
☛ Significant alterationin the follicular cell
architecture, characterized by cell crowding,
microfollicles, and dispersed isolated cells.
☛ Follicular cells are normal-sized or enlarged
and relatively uniform, with scant or
moderate amounts of cytoplasm.
☛ Nuclei are round and slightly
hyperchromatic, with inconspicuous nucleoli
☛ Colloid is scant or absent.
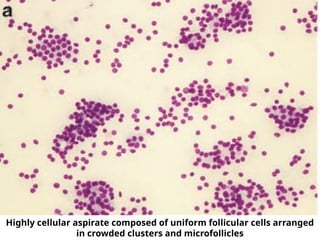
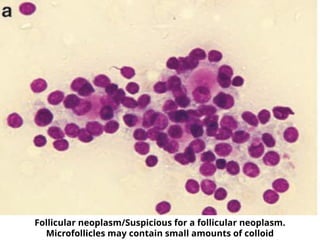
Follicular Neoplasm/Suspicious
for a Follicular Neoplasm
33.
Highly cellular aspiratecomposed of uniform follicular cells arranged
in crowded clusters and microfollicles
Follicular Neoplasm, HürthleCell
Type/Suspicious for a Follicular
Neoplasm, Hürthle Cell Type
☛ Exclusively (or almost exclusively)
Hurthle cells
☛ abundant finely granular cytoplasm
☛ enlarged, central or eccentrically located,
round nucleus with prominent nucleolus
36.
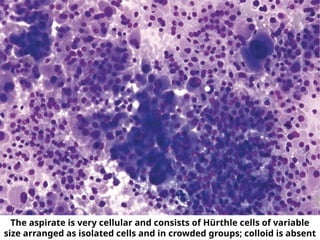
The aspirate isvery cellular and consists of Hürthle cells of variable
size arranged as isolated cells and in crowded groups; colloid is absent
37.
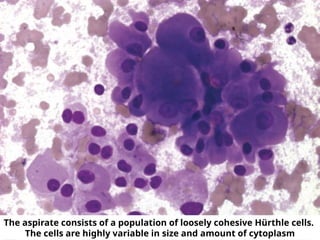
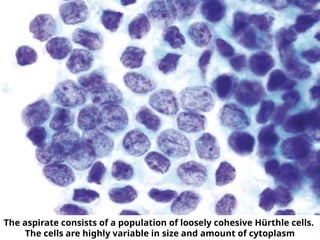
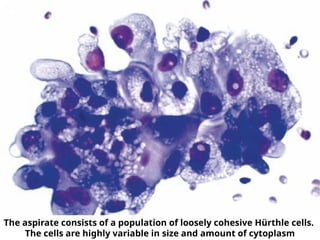
The aspirate consistsof a population of loosely cohesive Hürthle cells.
The cells are highly variable in size and amount of cytoplasm
Sub-categories
☛ Papillary ThyroidCarcinoma
☛ Medullary Thyroid Carcinoma
☛ Poorly differentiated Thyroid
Carcinoma
☛ Undifferentiated (Anaplastic)
Carcinoma and Squamous Cell
Carcinoma of the Thyroid
☛ Metastatic tumors and lymphoma
44.
Papillary Carcinoma
Thyroid
☛ Follicularcells are arranged in papillae
and/or syncytial-like monolayers.
☛ Swirling sheets (“onion-skin”) sometimes
seen.
☛ Characteristic nuclear features:
• Enlarged nuclei
• Oval or irregularly shaped, with marked
overlapping.
• Longitudinal nuclear grooves
• Intranuclear cytoplasmic pseudoinclusions
(INCI)
• Pale nuclei with powdery chromatin (“Orphan
45.
Papillary Carcinoma Thyroid
☛Psammoma bodies are sometimes
present.
☛ Multinucleated giant cells are
common.
☛ The amount of colloid is variable and
may be stringy, ropy, or “bubble-gum”
like.
☛ Hürthle cell (oncocytic) metaplasia is
sometimes seen.
46.
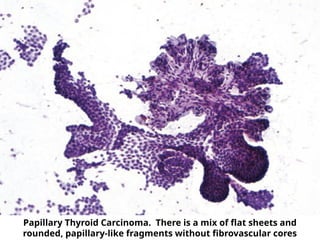
Papillary Thyroid Carcinoma.There is a mix of flat sheets and
rounded, papillary-like fragments without fibrovascular cores
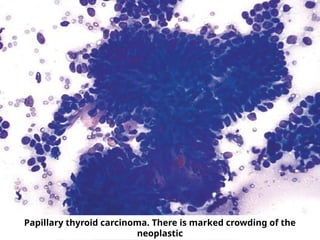
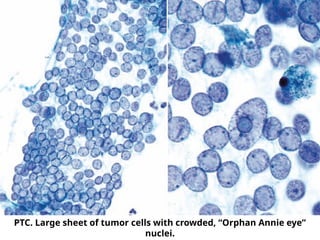
PTC. Large sheetof tumor cells with crowded, “Orphan Annie eye”
nuclei.
49.
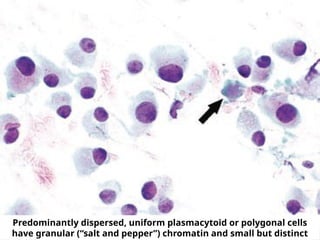
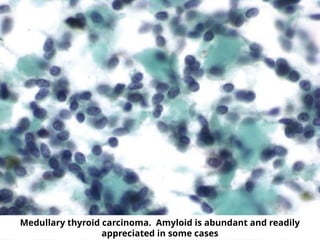
Medullary Thyroid Carcinoma
☛Moderate to marked cellularity.
☛ Numerous isolated cells alternate with
syncytial-like clusters in variable proportions
from case to case.
☛ Cells are plasmacytoid, polygonal, round,
and/or spindle-shaped, with moderate to
abundant cytoplasm, eccentric nucleus and
smudged chromatin
☛ The neoplastic cells usually show only mild
to moderate pleomorphism.
☛ Fragments of amorphous material - colloid
versus amyloid.
50.
Predominantly dispersed, uniformplasmacytoid or polygonal cells
have granular (“salt and pepper”) chromatin and small but distinct
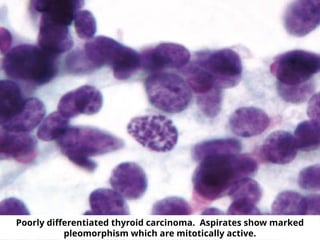
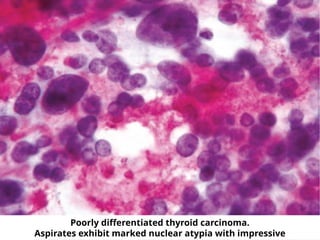
Poorly Differentiated Thyroid
Carcinoma
☛Cellular preparations display an insular,
solid, or trabecular cytoarchitecture
☛ There is a uniform population of
follicular cells with scant cytoplasm
(sometimes plasmacytoid)
☛ The malignant cells have a high
nuclear/cytoplasmic (N/C) ratio with
variable nuclear atypia
☛ Apoptosis and mitotic activity are
present
Undifferentiated (Anaplastic)
Carcinoma andSquamous Cell
Carcinoma of the Thyroid
Undifferentiated (Anaplastic)
Carcinoma
☛ Neoplastic cells are arranged as isolated
cells and/or in variably sized groups.
☛ Neoplastic cells are epithelioid (round to
polygonal) and/or spindle-shaped and
range in size from small to giant-sized.
“Plasmacytoid” and “rhabdoid” cell shapes
56.
☛ Nuclei showenlargement, irregularity,
pleomorphism, clumping of chromatin
with parachromatin clearing, prominent
irregular nucleoli, intranuclear inclusions,
eccentric nuclear placement, and
multinucleation.
☛ Necrosis, extensive inflammation
(predominantly neutrophils, “abscess-like”)
and/or fibrous connective tissue may be
present.
☛ Osteoclast-like giant cells (non-neoplastic)
are conspicuous in some cases.
☛ Neutrophilic infiltration of tumor cell
cytoplasm can be seen.
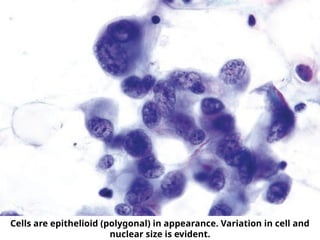
57.
Cells are epithelioid(polygonal) in appearance. Variation in cell and
nuclear size is evident.
58.
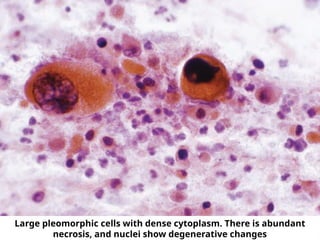
Squamous Cell Carcinoma
☛Cytologic samples are composed
almost exclusively of large,
pleomorphic keratinized cells.
☛ Necrosis may be present.
59.
Large pleomorphic cellswith dense cytoplasm. There is abundant
necrosis, and nuclei show degenerative changes
1. Nondiagnostic orUnsatisfactory
2. Benign
3. Atypia of Undetermined Significance or
Follicular Lesion of Undetermined Significance
4. Follicular Neoplasm or Suspicious for a
Follicular Neoplasm
5. Suspicious for Malignancy
6. Malignant
THANK
U
BSRTC