Downloaded 201 times

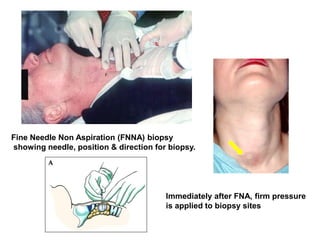
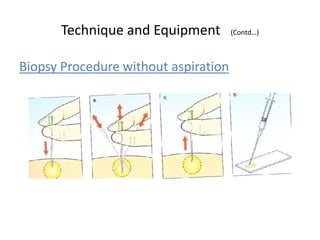

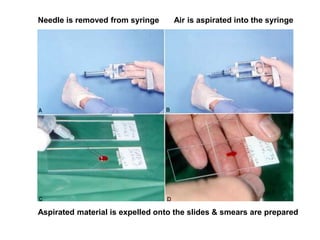

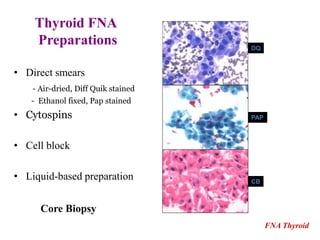


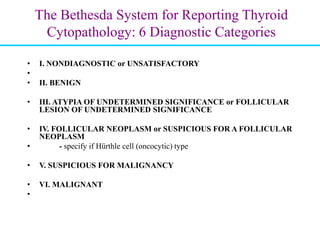
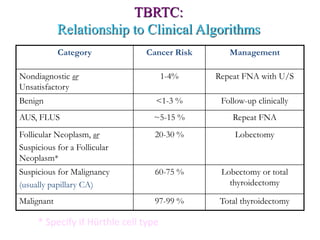
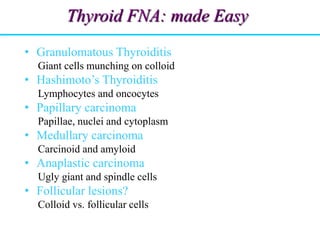


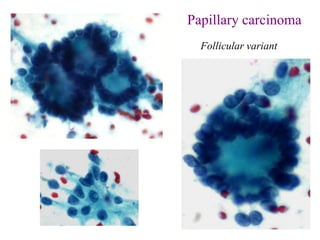





The document discusses the thyroid FNA procedure and diagnostic categories. It provides details on: - Performing thyroid FNA under ultrasound guidance using a 25 gauge needle with 3-4 passes. - Preparing direct smears, cytospins, cell blocks and liquid-based preparations from the aspirated material. - The Bethesda system for reporting thyroid cytopathology which includes 6 diagnostic categories and their associated cancer risks to guide clinical management. - Key cytologic features that help diagnose common thyroid lesions and cancers.