Downloaded 324 times





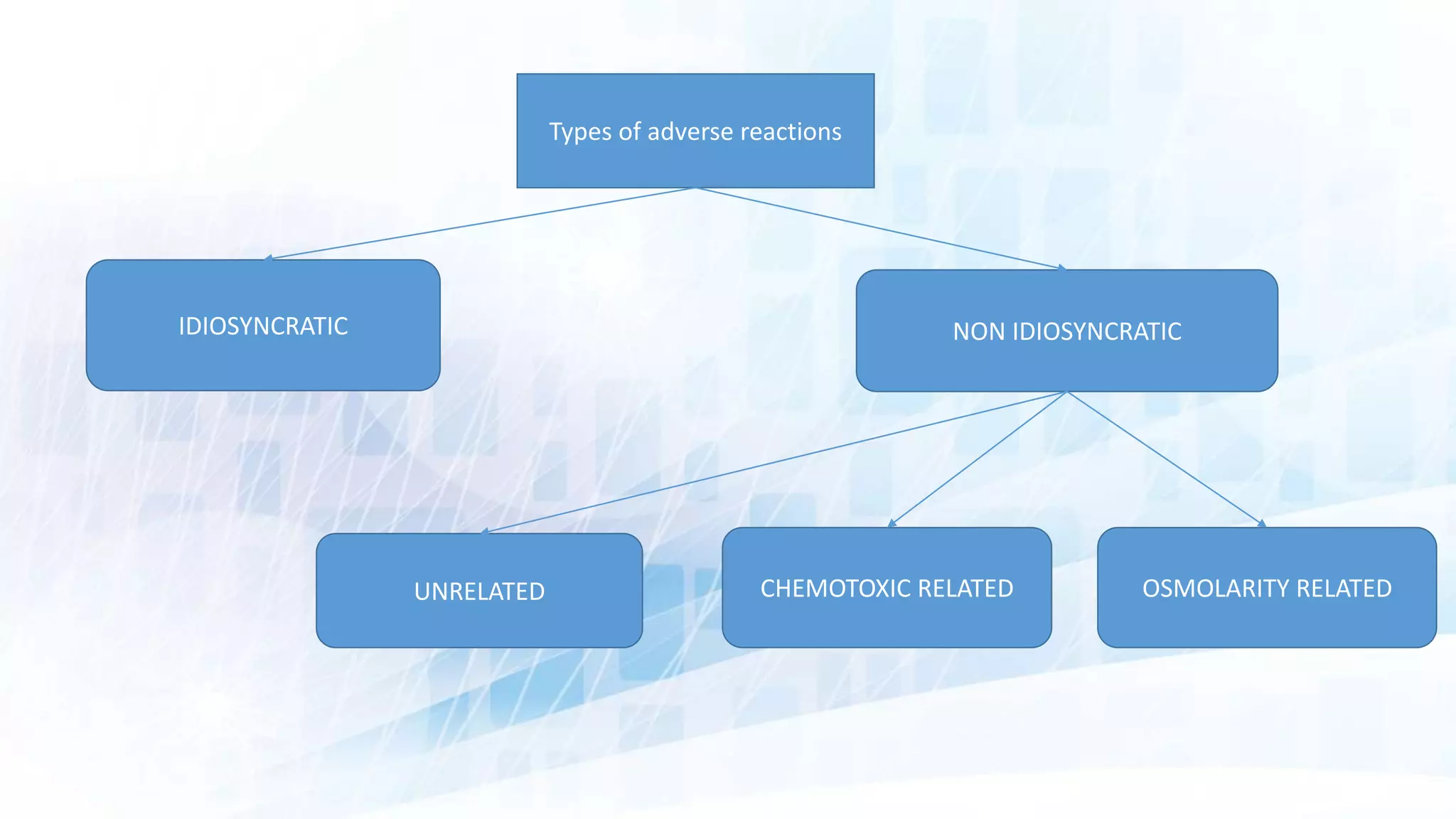































This document discusses contrast reactions and their management. It begins by stating that contrast reactions can range from minor to life-threatening. Proper preparation is needed to treat all potential adverse events. Risk factors for reactions include previous reactions, renal insufficiency, and medications. Reactions are classified as idiosyncratic or non-idiosyncratic. Idiosyncratic reactions are unpredictable and severe. Non-idiosyncratic reactions depend on properties of the contrast agent like osmolality. Management involves stabilizing airway, breathing, and circulation. Specific treatments are outlined for mild, moderate, and severe reactions like urticaria, bronchospasm, and hypotension.
Introduction to contrast reactions which can range from minor to severe, emphasizing the need for preparedness in treatment.
Key considerations for radiologists before administering contrast media, including patient risk assessment and appropriate preparation.
Description of common mild reactions and severe life-threatening reactions to contrast agents, highlighting unpredictability.Explains idiosyncratic reactions' unpredictable nature and management through risk reduction techniques.
Guidance on managing mild to severe idiosyncratic reactions, using the ABCDE approach for critical care.
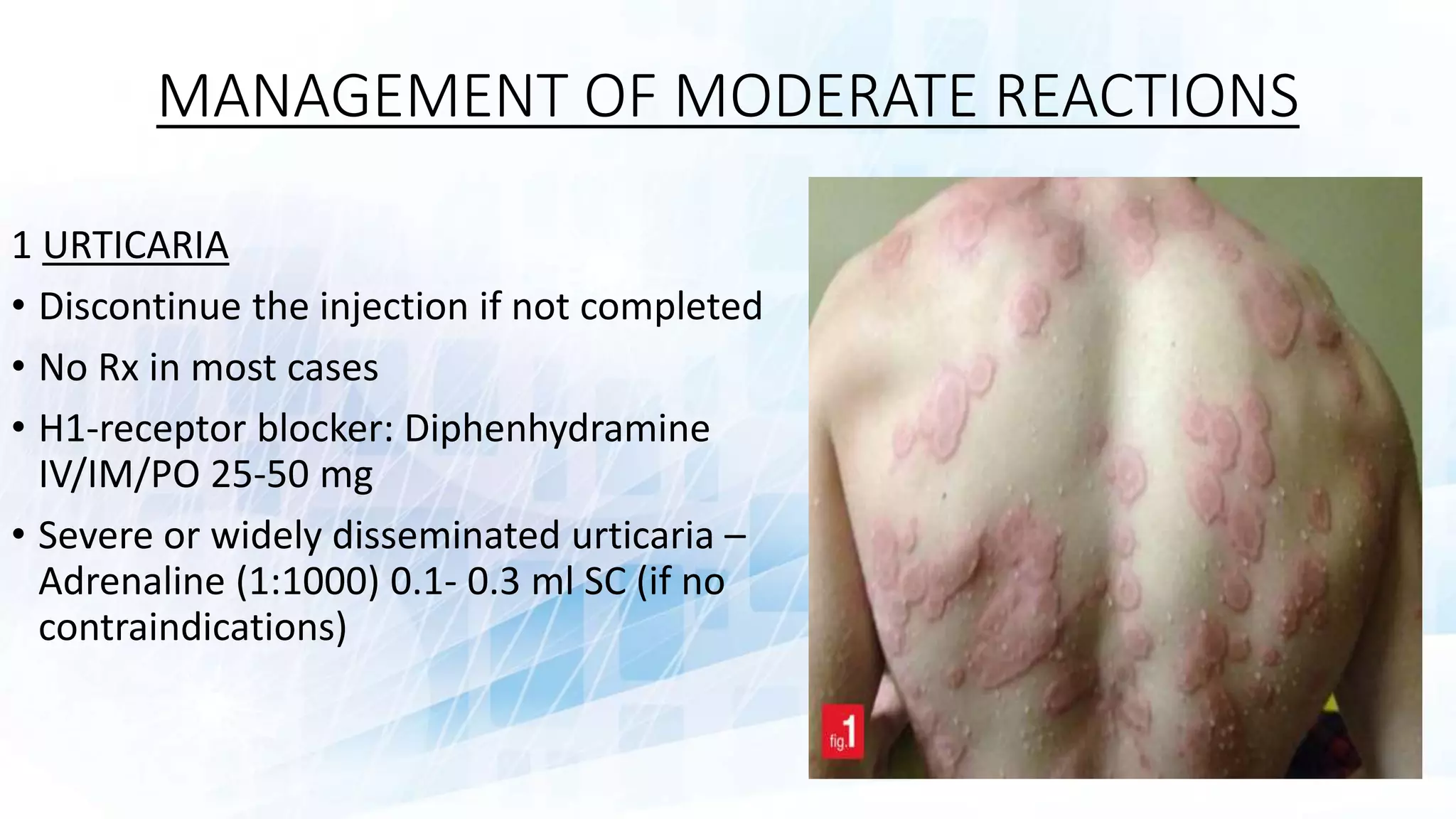
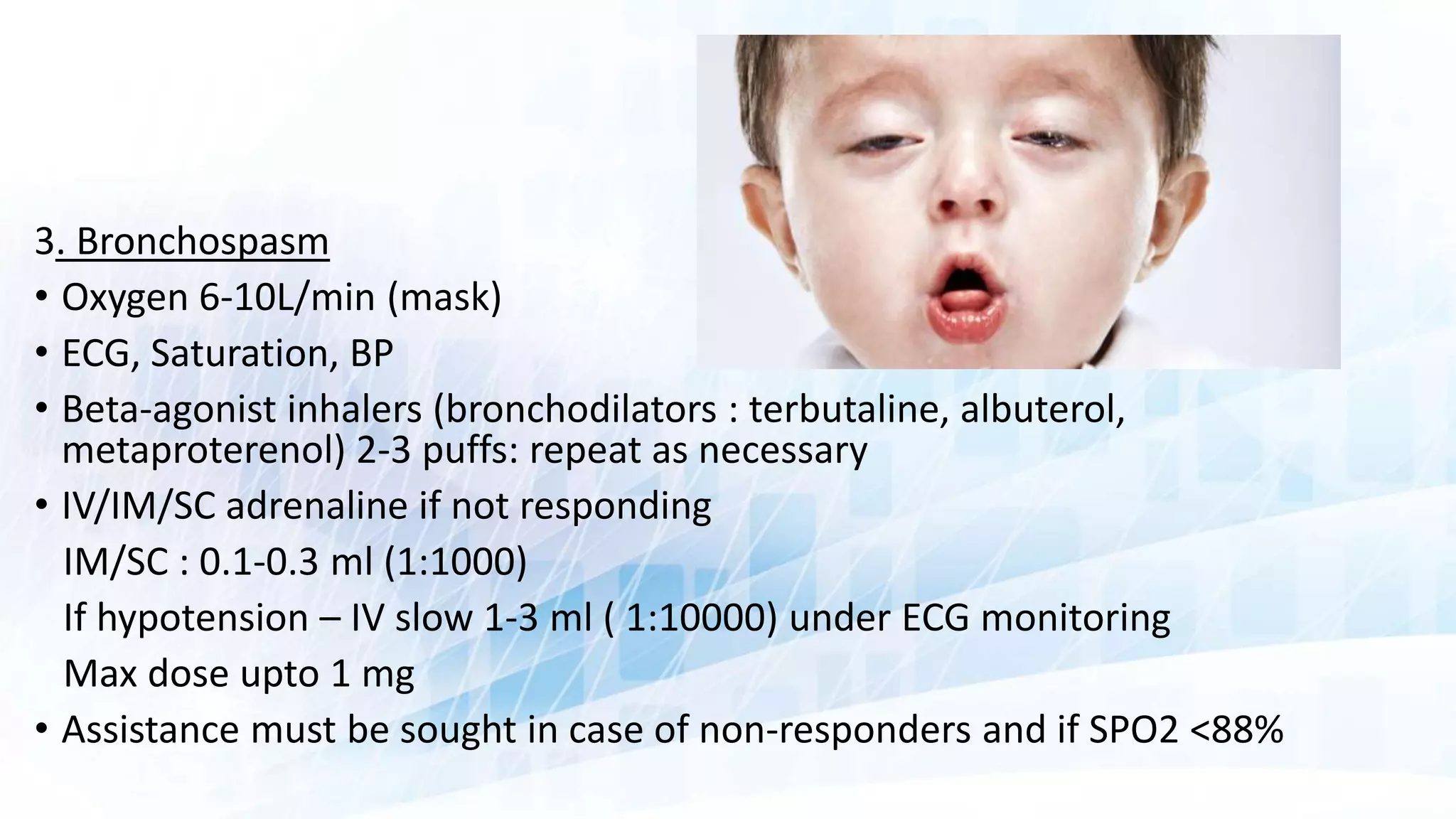
Detailed management protocols for moderate and severe reactions, including urticaria and hypotension treatments.
Explains non-idiosyncratic reactions including chemotoxic responses and vasovagal reactions.
Description of chemotoxic reactions, mechanisms involved, and effects on cardiovascular and renal systems.
Definition and clinical features of contrast extravasation with management strategies based on volumes.
Introduction to NSF, its association with gadolinium-based contrast agents and renal disease.
Identification of individuals at risk for NSF based on renal function and recent clinical exposure.
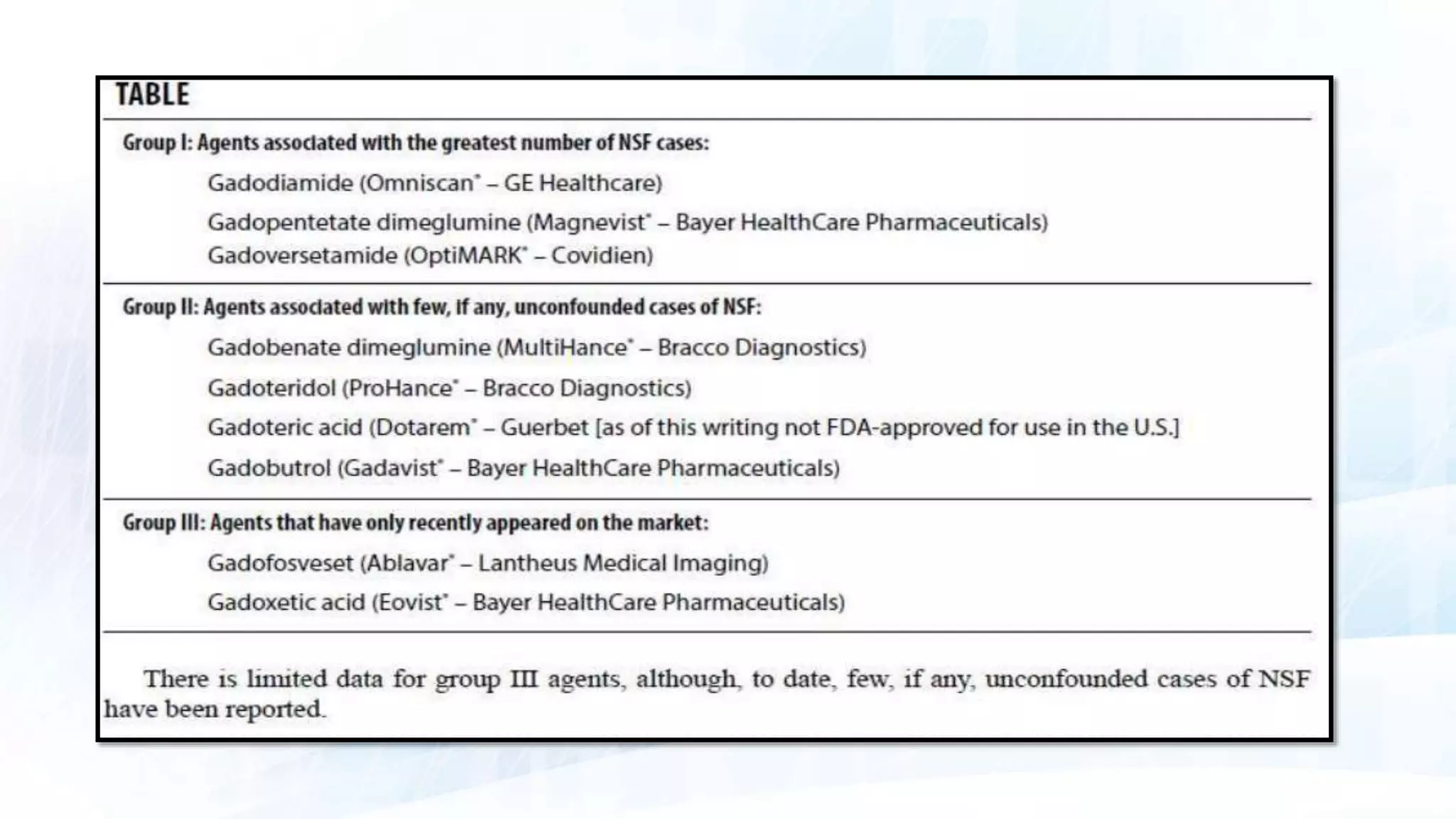
General recommendations for imaging patients at risk of NSF, discussing alternatives and precautions. Specific guidelines for GBCA usage in various patient groups to minimize NSF risk and manage exposure.
Other reactions and considerations related to GBCAs, including complications and contraindications.



































































