Downloaded 85 times

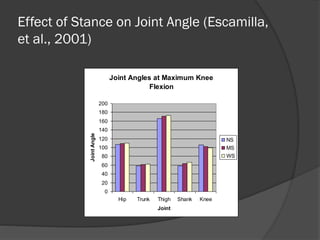

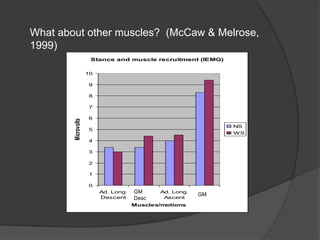
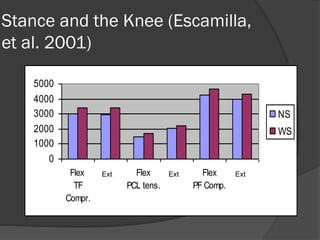
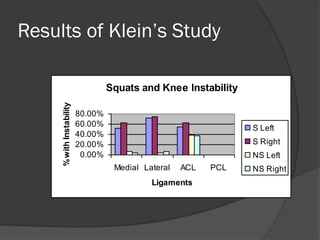
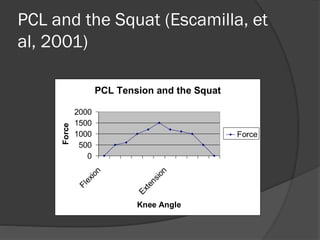

This document provides an overview of squats, discussing their benefits, myths, safety, technique, and variations. It summarizes research comparing narrow, medium, and wide stances, finding they have different effects on joint angles, muscle recruitment, and knee compression/tension but no stance is inherently riskier. While an older study linked squats to knee issues, more recent research has not replicated these findings. The squat places tension on the PCL during flexion but not the ACL. Proper form with hamstring engagement protects the knees.

















































































