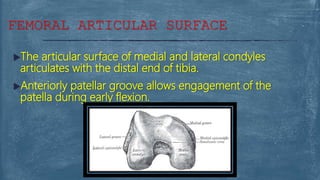
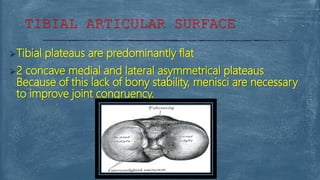
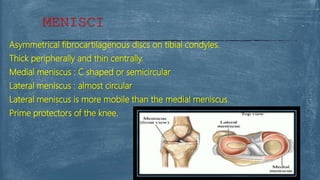
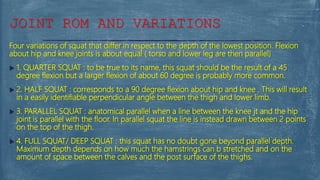
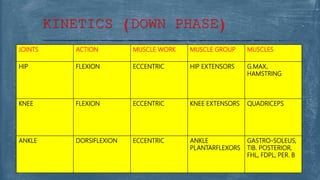
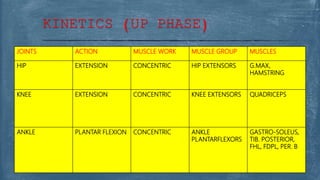
This document provides information about the knee complex, including its types of joints, articulations, structures, movements, and kinetics. It describes the femur and tibia articular surfaces, menisci, ligaments, bursae, and the patellofemoral joint. It also analyzes squatting movements, noting the roles of the hip, knee, and ankle joints during both the lowering and lifting phases, as well as variations in squat depth.