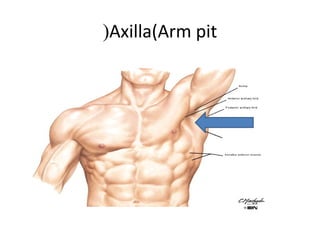
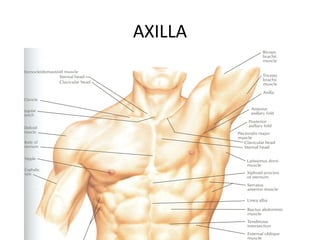
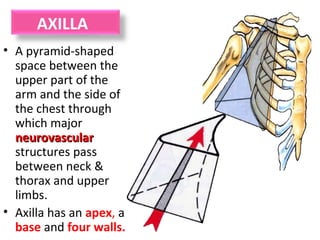
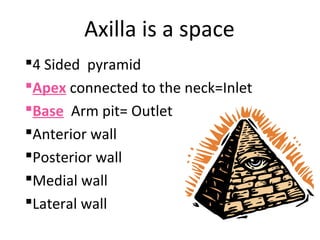
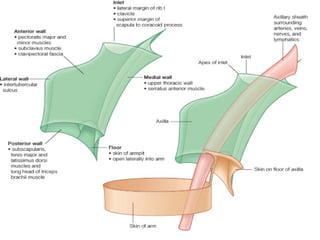
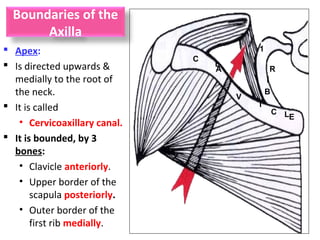
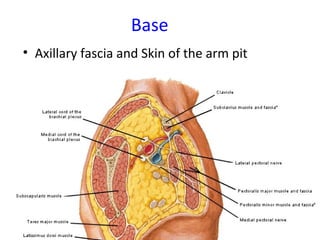
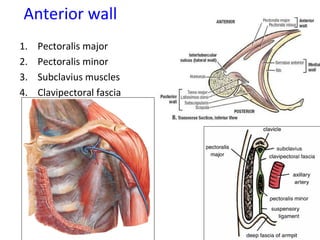
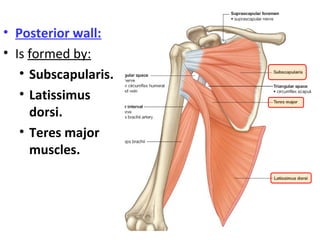
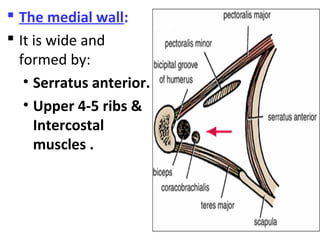
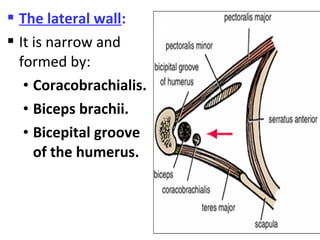
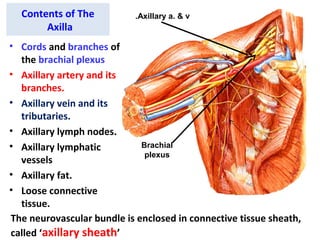
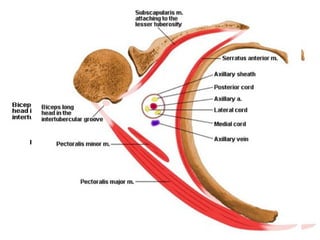
The axilla is a pyramid-shaped space bounded by the upper arm, chest wall, and scapula. It contains neurovascular structures passing from the neck to the upper limb, including the brachial plexus, axillary artery and vein, and lymph nodes. The walls of the axilla are formed by specific muscles like pectoralis major anteriorly and subscapularis posteriorly. The axilla allows for movement of the arm and transmission of major blood vessels and nerves.











































![Lecture 25 Intermuscular sapces and axilla [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture25intermuscularsapcesandaxillaautosaved-251110002658-47b36c78-thumbnail.jpg?width=640&height=640&fit=bounds)












































